It's Time to Take Action to Protect Vaccines and Start the Process to Throw RFK Jr. Out.
RFK Jr. is putting vaccines into a death spiral, and that's bad for all of us.

It’s a wild time for not only COVID vaccines, but vaccines in general right now.
Things are moving very fast, while somehow simultaneously moving very slowly.
For vaccine access in general, it’s moving very quickly… It’s difficult even to keep up.
However, if you are a regular reader waiting for Novavax, it’s moving slower than ever.
And everywhere I look, influencers are making it more complicated than it needs to be, which is, in fact, a conversation worth having about the power of influencers in general. Let’s put a pin in that for later, because we’re talking about the state of vaccines.
It’s not really a statement about influencers having power, but the ineptness of the people in power because of either nepotism, cronyism, or whatever “ism” that gives jobs to an acquaintance instead of someone who is equipped to do the work, which allows for social media “entrepreneurs” to drive the conversation.
Stories about how COVID vaccines will be limited have gone far beyond reality and are concocted to boost influencers’ subscriber base, while not providing accurate information or effective strategies.
This has even affected state governments and major corporations.
As this is the “People’s Strategist Newsletter,” that’s what we’re going to do…
Discuss a strategy that will actually be good for people.
We’re going to take a moment to cut fact from fiction and help you, the reader, navigate this situation. At the very least, trust me when I say, there’s a lot more we can do right now than is being advertised.
Things have been moving so fast that I wrote a rough draft on Monday, and by Wednesday, it was absolutely not up-to-date anymore.
We’re going to explain what’s going on and what you can do to help…
While also giving you a few tools that haven’t been on the chessboard yet.
Before we start, I would like to note that nothing in here is defending, in support of, or somehow being okay with how RFK Jr. is dismantling our public health systems.
We’re both trying to make it work now while also moving toward long-term solutions.
Sometimes, finding a functional solution in a time of crisis appears similar to an acceptance of the pressure we face, when there is still an opportunity to alleviate it.
I assure you that is not the case here.
Our group not only helped shut down RFK Jr.’s restructuring budget at appropriations but also played a crucial role in accelerating the yearly COVID vaccine release over the last two years, aiming to align the release with the school year and transition from a seasonal to a year-round strategy. This will be important later.
We’re a bit over four years into using these vaccines, and not only are we still learning how to use them, but, as Congress has been a dilapidated mess, none of this is legislated into law, which is why they even have the room to remove the vaccines in the first place, potentially. This wiggle room should not be ignored.
The idea of yearly vaccines is more of a courtesy than a required act, and last year, vaccines were released nationwide before ACIP issued an “official” recommendation.
That is, after all, what this debate is about: ACIP recommendations.
The only thing that makes it so your insurance will pay for these vaccines is if they are “ACIP recommended,” which is a legal requirement for insurance providers based on laws written by Congress. That’s really the only thing here that legally matters.
This is part of the Affordable Care Act, or as it is colloquially known, “Obamacare.”
So, it should be no wonder that Republicans might try to undermine it.
EDIT: Both New York, Minnesota, and Nevada have now allowed access in precisely the manner I lay out here. New York did it through the Governor’s office, and Nevada did it through the State Pharmacy Board. Hopefully, that will help alleviate some of the doubts people have about whether I am presenting the correct interpretation.
They would only have the power to do that if my interpretation is correct.
Make no mistake, ACIP is a hot mess with new members being appointed to drive around in that clown car in the last few days, with a meeting rapidly approaching in just a few weeks. Senator Cassidy is calling for this meeting to be postponed.
Though he kinda started this fire.
, chair of the Senate Health, Education, Labor, and Pensions (HELP) Committee, called for the U.S. Department of Health and Human Services Advisory Committee on Immunization Practices (ACIP) to indefinitely postpone their September 18th meeting.")
At the same time, Bernie Sanders is calling for RFK Jr.’s resignation, and over a thousand HHS staff are doing the same. While we should postpone this meeting for self-explanatory reasons, even if we did, it wouldn’t solve the recommendation issue.
Meanwhile, the actual limits are coming from CVS and Walgreens, which are the primary distributors of mRNA. However, in a confusing twist, they are requiring people to obtain a doctor’s prescription to access the vaccines in specific states.
Obviously, we all assume this is tied to specific legal requirements, right?
Buuuutttt… there’s a “small” inconsistency, and by small I mean enormous.
And I don’t mean that a prescription is explicitly never required for access.
They are limiting different states.
CVS is limiting access in the following states: CO, FL, GA, KY, LA, ME, NY, NC, PA, UT, VA, WV, MA, NV, MN, and DC: 15 states and the District of Columbia. So, 16.
Walgreens is limiting access in the following states: AZ, CO, GA, IN, LA, MO, MT, NM, NY, OR, SC, UT, VA, WA, WV, and WI…. also 16, but all states this time.
Do you see the problem here?
In total, it’s Arizona, Colorado, Florida, Georgia, Kentucky, Louisiana, Indiana, Maine, Missouri, New Mexico, New York, North Carolina, Pennsylvania, South Carolina, Utah, Virginia, West Virginia, Massachusetts, Nevada, Minnesota, Wisconsin, and DC…. making 21 states and DC.
There’s no consistency.
This is hypothetically tied to various state laws, which limit vaccinations to ONLY ACIP-recommended vaccines. The more I think about this, the more I hate it.
The reason it’s inconsistent is that none of this is based on CLEAR law; it seems it’s an issue with state liability for administering the vaccines outside of the ACIP recommendations, so the threat is purely from the states themselves.
Some states are already taking action to this effect.
New Mexico issued a public health order.

Pennsylvania is taking a clear stance on the issue and breaking from ACIP recommendations.
The problem is that this is already leading to significant confusion because these health orders do not force insurance to cover them. That means that while you can access them, you may have to pay out of pocket.
This will limit access to those who need these vaccines the most.
It will also limit access for programs that distribute vaccines to children at no cost.
If this plan is our new neutral, then the antivaxxers win.
This all comes down to a liability issue, which, even if every state changes its laws or makes exemptions in some way, as they should, does not necessarily answer the question of whether insurance will cover it.
The strange thing is that a doctor’s prescription doesn’t negate that liability, so I am still unclear why Walgreens or CVS sees that as a solution. Especially since federal protections for administering these vaccines were extended for several years.
It’s already been stated that some insurance companies will choose how to cover them plan by plan, but that can quickly become case by case.
If you haven’t noted, everyone is making things up on the fly, and this is what the antivaxxers want… whether it be altering access, or confusing people in general.
Ultimately, their goal is to limit access to vaccines, which will reduce demand, and over time, capitalism wins because there’s too much waste, and it will be viewed as not profitable… Which, to be clear, is a silly plan, but that’s who we’re dealing with.
And as silly as it sounds, this is a problem we’ve already faced in multiple countries with Novavax, where access was limited and not advertised. Then they turned around to say there was no demand. The problem now is that pro-vaccine advocates are doing the heavy lifting for the antivaxxers, telling people they can’t access these vaccines…
When that is not actually true, if we followed regulations as they stand.
Currently, we need to address the immediate accessibility of these vaccines, the long-term recommendation issue, and ensure that insurance coverage remains consistent throughout. While also figuring out how to get RFK Jr. out of a job.
We will almost certainly have to deal with some limits on access during that time.
Fortunately, we have enough wiggle room to make it work in the meantime.
While you might not like our access to COVID vaccines being limited to “wiggle room,” this is what folks seeking Novavax have had to deal with under both administrations… But that’s not what we’re going to talk about right now.
The idea you should focus on, as I explain everything else, is how close we are to removing RFK Jr. altogether because it’s not just the Democrats with a bone to pick.
Almost no one is aware that RFK Jr.’s HHS restructuring bill got shut down in appropriations with a vote of 26-3 to move on without his changes.
He’s coming off a major “L.” The Republicans aren’t happy with him either.
He’s basically pulling this off because he’s viewed as Trump’s pet.
… Changing paces, what if I told you that all COVID vaccines are automatically ACIP-recommended regardless of the year-to-year recommendation?
RFK Jr. said, “Talk to your doctor,” which has been interpreted as get a prescription, but that’s a simple misunderstanding of the niche regulation.
Say what you want about him, the FDA Director already understands the solution.

I’m not a fan of this guy, but what he said is not inherently false.
It’s one thing to hear it from me; it’s another to listen to it from the guy in charge, and once everyone understands how this works, we can push for clarity.
It sounds made up, but the process that allows this was a safeguard established by a combination of our group’s efforts over the last few years to make it as easy as possible for people to start Novavax with three in a year to receive maximum protection, and the former ACIP to protect all COVID vaccines in general.
If you haven’t questioned me up to this point, then I’m sure that’s what did it.
However, we have the receipts in the form of presentations we gave to prove it.
The problem we are facing is that the “vaccine skeptics” feel that ACIP recommendations become soft mandates when getting all the ACIP-required vaccines becomes a requirement of your job.
When they talk about “mandates,” I think that’s what they are referring to.
And I say “I think” because it’s like trying to translate stupid.
The point is that if we can find a way for Walgreens and CVS to accept this form of recommendation and make it the primary method for people to receive COVID vaccines, then they will be instantly covered by insurance, and access won’t be limited.
Most importantly, this process uses a “self-attest” system.
If we use the self-attest system, it would be ACIP-recommended enough to be covered by insurance, but not ACIP-recommended enough to become a “soft mandate…”
And somehow, oddly offers more access than we had in the previous administration.
Under these guidelines, anyone would be able to receive a COVID vaccine as long as it is two months after a previous one. Unless someone is starting with Novavax for the first time, then no one needs a COVID vaccine that often.
Accepting this strategy would mean that all COVID vaccines are covered by insurance, available to you as frequently as you want, as long as it’s been two months since the last one, all while using a self-attest system, and not creating a soft mandate.
So, let’s get moving before you have time to second-guess the decision to read further.
Let’s start with the ‘Shared Clinical Decision-Making Guidelines.’
Do you need a prescription?
Do you need to claim you are immunocompromised?
You can do those things if you’d like, and in some cases, it may make things easier.
However, not everyone has easy access to a doctor, and due to HIPAA, you cannot be required to disclose your health status except under certain circumstances…
These guidelines were designed with that in mind to remove those circumstances.
There is a chance you will be handed a piece of paper that may require a box to click, stating you are immunocompromised or at risk of severe COVID. Still, hopefully, we can narrow the question down to “are you using the shared clinical decision-making guidelines?” But as we are all aware, they reuse old documents for way longer than they should, so that’s just a thing we may have to deal with.
To clarify, it has been discussed at great length at VRBPAC meetings that stating you are immunocompromised, even if you are not, is specifically how the rules were set up to allow access to additional Novavax doses. It’s not really lying because it’s intended to be used that way, only to make it easier for pharmacists to allow access.
It sounds ridiculous, but making things “idiot proof” involves bending definitions.
Putting all COVID vaccines on this list last year was part of our solution for the problem of allowing for a new priming series. So, in a way, we are recycling solutions, but it works out now so that it helps everyone who wants COVID vaccines, rather than just those who want a new priming series of Novavax for maximum protection.
We’ve presented a total of five times at VRBPAC:
VRBPAC Meeting: June 15th, 2023 - COVID
VRBPAC Meeting: March 5th, 2024 - Influenza.
VRBPAC Meeting: June 5th, 2024 - COVID
VRBPAC Meeting: Sept. 20th, 2025 - Pertussis
VRBPAC Meeting: May 22nd, 2025 - COVID
We fought to change the requirement to claim immunocompromised, and later, the documentation removed the requirement to claim immunocompromised altogether. However, it does still exist in some documentation from last year, leading to confusion.
Here are the guidelines for the 2024-2025 season, which serve as the basis for RFK Jr.’s claims that anyone will have access to these vaccines.
Even if you hate RFK Jr. and hate this process, you want these rules preserved.
Before you proceed, please note that these guidelines apply to children who are NOT moderately or severely immunocompromised.
So, not the group at risk of severe COVID who maintain a general recommendation.
This essentially means these rules apply to everyone in some capacity.

Will documentation be required?
No. Well, at least it shouldn’t be if they were following the regulations as they stand.
These are the rules for immunocompromised people, but it explicitly says that you can “self-confirm,” also known as “self-attest,” which means it’s on the honor system.
 because of a medical condition or if you received medications or treatments that suppress your immune system. You can self-confirm if you are moderately or severely immunocompromised. This means you do NOT need documentation to receive a COVID-19 vaccination you are eligible for.")
“You do NOT need documentation to receive a COVID-19 vaccine you are eligible for.”
This is where wording from different documents can become confusing, but it is overwhelmingly stated that you can self-attest to a status that allows for COVID vaccine access. It makes that clear in all eligibility capacities…
It’s a strange fight for eligibility when you are in charge of deciding for yourself.
Essentially, you are deciding your own eligibility, after discussing it with “whoever is in charge of your healthcare”… probably you, and they even dramatically capitalized “NOT” to emphasize the fact that you do not need documentation or a prescription.
Technically, the complete list of “healthcare providers” is “primary care physicians, specialists, physician assistants, nurse practitioners, registered nurses, and pharmacists,” but, again, no documentation is currently required.
That means that access to these specific people is not a limitation.
But will insurance cover it?
Yes, absolutely.
We’ve been doing this for a year already, so that folks can access a new priming series.
. This coverage requirement includes shared clinical decision-making recommendations when they have been adopted by CDC and are listed on the immunization schedules.")
“With respect to the individual involved” sounds an awful lot like shared clinical decision making, but at this point, I’d be happy to get an objective opinion.
Didn’t RFK Jr. already tell us the recommendations were changed?
Technically, he has only expressed his intention to change the recommendation, but the actual ACIP recommendations haven’t been changed since 2024.
; 1118-1123 Use of Additional Doses of 2024–2025 COVID-19 Vaccine for Adults Aged ≥65 Years and Persons Aged ≥6 Months with Moderate or Severe Immunocompromise: Recommendations of the Advisory Committee on Immunization Practices — United States, 2024 Print version MMWR, September 10, 2024. Vol 73 (37);819-824 Use of COVID-19 Vaccines for Persons Aged ≥6 Months: Recommendations of the Advisory Committee on Immunization Practices — United States, 2024–2025")
There is an interim guidance page, but it’s incomplete, and many links are dead.

Now, that being where things stand now, does not mean that’s where they will be, but we will get to that in a moment, because more than COVID vaccines are at risk.
For right now, this all comes down to CVS and Walgreens establishing the status quo that all COVID vaccines are administered according to the shared clinical decision-making guidelines. Ensuring that insurance pays for it, and access will be available regardless of variant changes. As long as the FDA approves the variant selection and batches, then CDC meetings should not hinder access to the public.
Accepting this now would benefit us in the future, regardless of who is in charge, while also providing a specific point of pressure to ensure access.
This would also go a long way to help us be more nimble and respond to COVID as it mutates, regardless of how the CDC sets up its meetings earlier in the year.
This way, it would only require approval from the FDA to change variants without needing Congressional members to actually do their jobs.
We’ve already determined these platforms safe, though at variable levels of protection, so reapproving them every time the variant changes is more theatre than safety.
And it’s all just a matter of groups like CVS and Walgreens setting the new status quo.
If we adopt this now, it will allow more access, the antivaxxers get their dog and pony show that vaccines are being limited, and vaccine skeptics lose their soft mandates.
It’s weird because it’s possible everyone wins.
This probably doesn’t match up with what other influencers are saying.
Which is why it’s essential to keep track of the misleading claims being said and have the correct response for each individual issue:
A doctor’s prescription will be required.
At no point has any regulator made that claim; however, there has been confusion over whether shared clinical decision-making requires a conversation with your doctor or your “healthcare provider,” which is a broader interpretation. Many are interpreting this as requiring the creation of documentation of this conversation in the form of a prescription, and that is explicitly not the case. So, unless they change the shared clinical decision-making guidelines (which badly needs an abbreviation), that is incorrect at every step and should not limit access.
Around 24 states and DC are limiting access by prescription under the pretense that these are not ACIP-recommended vaccines. In some cases, state liability laws will come into effect, preventing their distribution. States are trying to find workarounds that alter their state laws in relation to ACIP.
This is simply wrong at every level. I cannot express how incorrect this is. Under the shared clinical decision-making guidelines, these remain as ACIP-recommended vaccinations. No additional changes should be necessary. Changing state rules to follow ACIP guidelines is a slippery slope, potentially leading to red states limiting the enforcement of laws that mandate insurance coverage for vaccines. We’re better off trying to fix ACIP than we are trying to alter every individual state’s laws. Anything more than an Executive Order to protect liability is going too far to enable distribution because it might negatively affect other aspects of access.
Insurance will not cover these vaccines.
This is obviously incorrect, again, unless the guidelines are changed. Altering the greater recommendation will not impact this unless they are removed from the shared clinical decision-making guidelines. I have been personally holding people’s hands through this process for over a year.
We don’t know what criteria will allow access to vaccines.
This is a bit of a no-brainer if you read this far. However, since people will still be in doubt for various reasons, here’s the list of conditions that allow anyone access, according to the recommendations they claim to want to make. This is not a list of conditions that allow access, but rather a list of high-risk conditions that put you at the highest risk for severe COVID. Also, important to note two things: 1. This is not an exhaustive list; it simply indicates who should automatically have access. 2. You are not required to disclose any condition to access these vaccines. Also, bonus, while they are trying to limit vaccines to pregnant people, pregnancy is still listed as a high-risk condition for severe COVID.
In two weeks, the illegitimate ACIP is meeting again, and they may alter the recommendation. Vaccine companies are waiting to distribute based on how that meeting might go.
This is a genuine concern.
We should start by stating that the removed ACIP had the fewest conflicts of interest of any recent ACIP, as our group informally removed all but one ACIP member by contacting them directly at their academic email addresses.
They even expressed their frustration with us during a meeting.
To say the former ACIP represented twenty years of corporate malfeasance, as RFK Jr. has, is an absurd claim, given that all the members were replaced the previous year.
And it’s not just this last ACIP… Conflicts of Interest (COIs) are at a historic low for both the ACIP (CDC) and VRBPAC (FDA).
 prevalence rates for all meetings in that year. The lines are the quadratic fitted line for the Advisory Committee on Immunization Practices (ACIP) and a fitted linear regression line for the Vaccines and Related Biological Products Advisory Committee (VRBPAC). Average prevalence of COls in a given year was calculated as the unweighted mean of meeting-level COl prevalence rates for all meetings in that year (ie, prevalence was not weighted by the number of meeting attendees).")
So, what are our options?
We get CVS and Walgreens to change their policy, then what?
Not everyone will understand the shared clinical decision-making guidelines, and while they will enable access, these additional steps will still reduce uptake.
We could try to bend the rules in all the states, or we could try to fix ACIP.
We could also do both.
As far as states are concerned, getting the Governors to sign Executive Orders that will protect pharmacists from the liability of state laws will likely enable access…
So, will contacting the State Pharmacy Board.
Or states like New Mexico are implementing rules that allow access in other ways.
The most important thing a state can do is remove limitations for any group to access all COVID vaccines regardless of federal stipulations.
Really, this process only exists for clarity, and it’ll be easier to resolve this statewide.
Since the shared clinical decision-making guidelines are so intentionally ambiguous, it’s questionable if this is necessary at all. However, it is something that news agencies will discuss, letting people know that these vaccines are accessible. While some people are surprised by this problem, we were aware that it could be a concern.
This is one of the reasons we advocated for not updating vaccines this year, as they had already been approved. Technically, it’s not a new vaccine, and it would likely have a more streamlined approval process to remain on the market.
Not only that, but it was also the best variant option.
Just a quick side step on whether JN.1 is actually the best variant choice… but don’t worry, I’m going to explain the process to reinstate ACIP, impeach RFK Jr., and put all this madness to an end. You can read our entire 2025 VRBPAC presentation here.
Last year, we were in the same boat, choosing between what is known as a “leaf on the tree” or the “trunk of the tree,” the former referring to a random variant, and the latter referring to the primary variant from which all the current subvariants emerged. You can read our entire 2024 VRBPAC presentation here.
There is a common misconception that we want to get as close as possible to a circulating variant; however, several issues arise.
With the primary problem being that aiming for a current variant means that it will likely have circulated out by the time manufacturing can be complete, even for mRNA, and that brings us to the second problem, where the new variant will likely have immune evasion to the antibodies created by both the previous variant and the vaccines you just released.
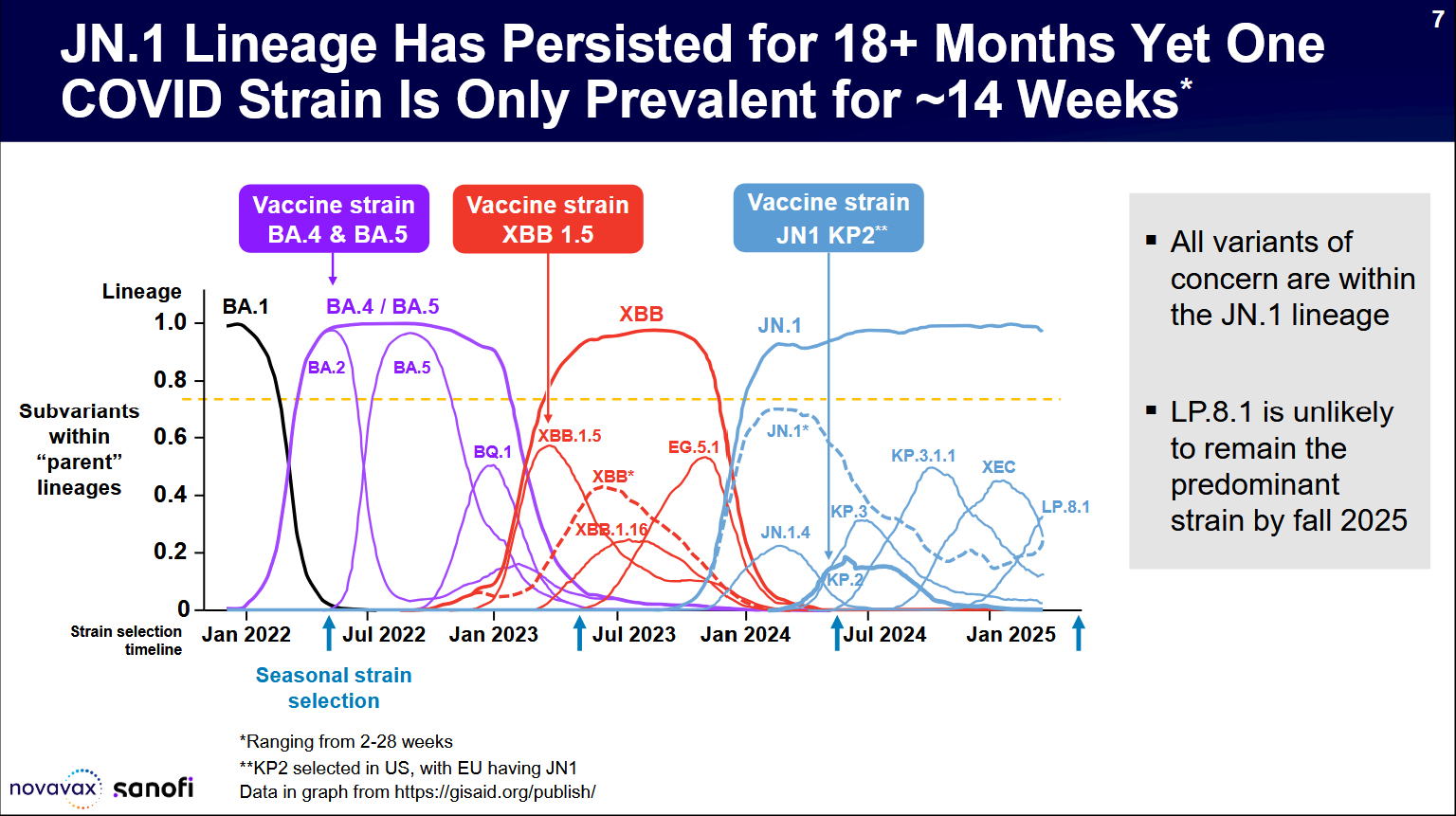
The point that is repeatedly emphasized is that each individual variant has less in common with the other variants than it does with the parent variant.
And though we did not use JN.1 mRNA in the US, we did use it internationally.
This provided us with some stark data on the matter, with the JN.1 mRNA far outperforming the KP.2 vaccines. It’s not even close.
JN.1 is in blue.

However, this is from last year. What about variants now?
Here’s a demonstration of the current variants. This was presented at the May VRBPAC meeting. You can see that XFG, NB.1.8.1, and LP.8.1 are all within 1-2 antigenic units, which is a standardized measurement of antigenic distance.
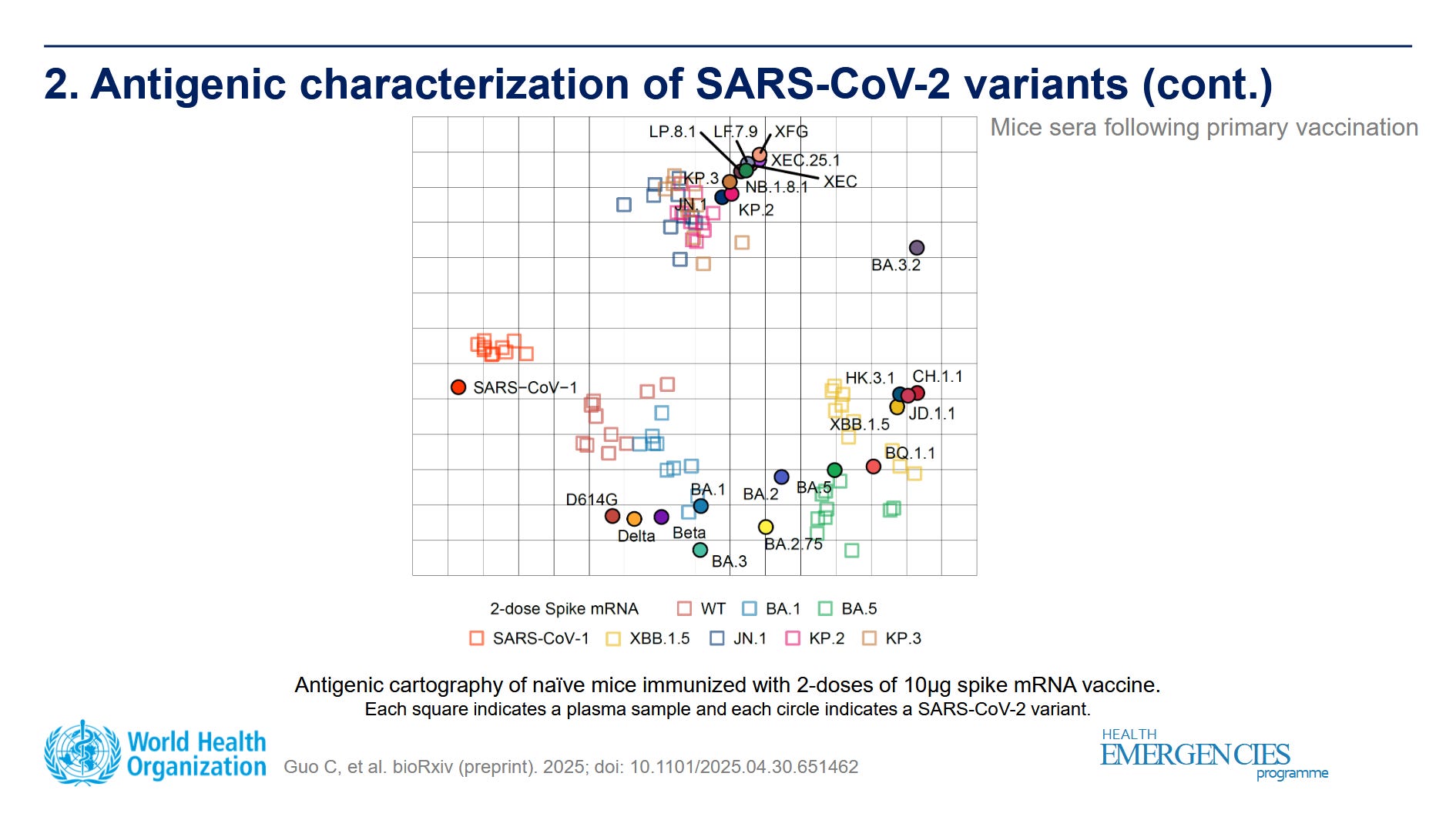
What you might miss in this chart, though, is that the actual vaccine sera responses do not line up directly with the variants themselves, and all of the responses end up closer to JN.1 than they do their intended target.
This is really important to note because people often seem to think that it’s like driving to a location in the real world; do you want to drive and park two blocks away?
No, of course not, I want to park as close as possible.
Well, in immunology, you are parking “two blocks” away, regardless. Which means we are better off planning for the walk than denying that it’s part of the process.
Also, sticking with JN.1 would have let us skip all this needless drama; we could have updated everyone’s memory response, and we could also begin the process to move to a year-round COVID response instead of a seasonal one, as COVID does not peak in the winter season alone and is actually far more likely to peak in the summer than more traditional respiratory viruses, as we are seeing now.
Seasonality, as observed during the winter season, when we are more susceptible to infection, does not significantly impact COVID-19 spread, with waves regularly occurring during warmer months.

It’s worth noting that VRBPAC in 2024 took place in June, whereas VRBPAC in 2025 occurred in May. If we continue to move up VRBPAC next year, then we can have vaccines out before the school year starts. This means we need VRBPAC in April to plan for a July/August release, rather than May for an August/September release.
You can watch the previous VRBPAC meeting, starting with my public comment presentation, and observe the conversation our presentation started regarding not updating the vaccines this year.
Ultimately, only three of the nine members thought updating was the right choice.
Maybe it was four, but no consensus was reached on the concept.
It was ultimately Vinay Prasad’s CBER that made the call to update to LP 8.1.
So, try to remember that when folks in the COVID-conscious community discuss LP.8.1 as the better choice because it is “more updated,” they are actually following through with Vinay Prasad’s plan from the new CBER.
Which is funny because Prasad is making the same mistake that Peter Marks made last year, which goes to show that it doesn’t matter who is in charge; they still make the same mistake because the same groups are pulling the strings.
Okay, Don, get back to the Impeaching RFK Jr. talk.
I completely understand if you are not up-to-date with our group’s work and therefore might share opinions with this individual.

We are a bit further along with this than this perspective might suggest…
On a side note, this highlights the issue of influencers exploiting the trust they’ve built with their followers and manipulating the parasocial relationships created on social media. This person is totally unaware of the work we have done while following me at the same time. The larger influencers are, for some reason, pretending this all didn’t happen, and consequently, neither does this individual.
I should point to Taylor Lorenz’s recent article on the pay-to-play political influencers and how this is not an abnormal event unique to politics.
While much of her article is framed as influenced by the Democratic Party, it’s actually about influence OVER the Democratic Party. This type of influence exists in any high-dollar situation, and COVID vaccines are technically higher on the economic ladder than control of the Democratic Party.
In other words, pay-to-play influencers for topics related to COVID are likely to be even more common and require even fewer disclosures.
Instead of pointing fingers, let’s take a look at the work.
Here are the previous articles on these actions, but please note that we are also hosting ‘Brace for Impact’ to activate our listeners twice a week with calls to action.
Brace for Impact is Tuesdays and Thursdays, starting between 6 and 7 pm Pacific.
January 29th, 2025
March 25, 2025
April 3, 2025
April 16, 2025
May 12, 2025
June 20, 2025
June 24, 2025
July 1, 2025
July 8, 2025
August 8, 2025
What does this all mean?
We were taking a victory lap because, after a multi-month process, we were able to protect public comment and also shut down RFK Jr.’s HHS restructuring budget in the appropriations committee. This was not covered by any major media group that we have identified, other than STAT News.

On the surface, this might not seem like a big deal, but it’s a huge deal.
The appropriations committee, like all committees, is controlled by Republicans.
That means that the Republicans had to decide that his plan was a bad idea.
And only three Republicans on the committee voted against moving forward without his additions. Meaning that only three Republicans on the committee supported his changes, but he only lost that support after events unfolded in Congress.
So, what happened?
Well, RFK Jr. perjured himself multiple times in Congressional hearings.
We’ve already seen Bill Clinton famously impeached for perjury, and make no mistake about it, committing perjury to Congress is grounds for impeachment.
Now, this, combined with the reality that Republicans voted against his restructuring budget, means that there are enough combined House members who are against what RFK Jr. is doing to push for formal impeachment.
Will it happen?… Well, it could.
It also becomes leverage for the upcoming ACIP meeting, especially given RFK Jr.’s practice of altering recommendations without consulting an expert first.
RFK Jr. has more congressional hearings coming up and multiple ethics complaints.
I expect to see him perjure himself more because, as far as I can tell, he doesn’t seem to know where he is from meeting to meeting. Watching him deny conversations we had observed him having a few weeks earlier was a new one for me personally.
The truth is that getting him impeached will take a minute, but the tools to make it happen are available to us, and we should get started.
Okay, but what about ACIP?
Senator Cassidy is currently advocating for the next ACIP meeting to be postponed.
You’ve already seen this, but it’s a long article, so it’s probably good to revisit it.
, chair of the Senate Health, Education, Labor, and Pensions (HELP) Committee, called for the U.S. Department of Health and Human Services Advisory Committee on Immunization Practices (ACIP) to indefinitely postpone their September 18th meeting.")
However, this will disrupt access in multiple states until either the ACIP can meet and officially recommend them or the individual Governor signs Executive Orders limiting liability to people who administer the vaccines, or a similar act is taken by public health officials, as in New Mexico.
Alternatively, we could establish a new status quo with the major corporations.
Although concerns remain about insurance coverage, leaning into Shared Clinical Decision Making is the best approach for at least the remainder of this year.
Though that’s a short-term plan, and while that’s helpful, we need a real solution.
This is where the Senate bill to legalize ACIP comes into play.
Legalizing ACIP and reinstating former members should be extended to include reinstating the former CDC Director, as well as preventing such firings in the future.

The bill is co-sponsored by U.S. Senators Angela Alsobrooks (D-Md.), Martin Heinrich (D-N.M.), Ben Ray Luján (D-N.M.), Jeff Merkley (D-Ore.), and Raphael Warnock (D-Ga.).
As the CDC Director is now Senate-confirmed, the White House should not have the ability to fire a CDC Director without proper cause that is presented to the Senate.
Republican Senators who are unwilling to impeach RFK Jr. for perjuring himself may be more willing to enforce the ACIP membership directly.
However, the issue is that Trump would have to sign that bill into law.
Perhaps we get lucky and Vance signs it into law.
This is why impeachment of RFK Jr. should be a reasonable possibility, because it doesn’t require the President’s signature.
We need to do all of this because we are not only having troubles with COVID vaccines, but two workgroups of fringe antivaxxers have been set up to call into question various vaccines. This is just their first stop.
One workgroup is focused on COVID vaccines, and while I would like a greater conversation about vaccine injury from mRNA, this is not the group we want to lead it.
Even as a proponent of Novavax, in this situation where it is likely to leave Novavax in a stronger position, this is not how or who we want doing this.
The second group focuses on Childhood vaccines in general and makes recommendations to Congress every two years. This itself is not something to be afraid of, because we are on the verge of improving several vaccines typically received by the entire population during childhood.
However, that’s not what the people selected are focused on; we should be worried.
But where does that leave us?
We have two weeks to get ACIP put on hold, take the state’s route, reinstate the former ACIP, or get the current ACIP to recommend them broadly.
While at the same time, open up access to COVID vaccines without an ACIP meeting.
However, we actually have one option that could help us more than the others.
CVS and Walgreens are dominating this conversation based on incorrect information. Most importantly, a prescription is NEVER required, and they are not following ACIP recommendations as they stand. These vaccines remain ACIP-recommended from year to year due to the shared clinical decision-making guidelines.
Additionally, we should push through the bill to legalize ACIP membership so it can’t be used as a political weapon, all while starting RFK Jr.’s impeachment proceedings.
However, these are niche regulations that not everyone seems to be aware of.
COVID vaccines of all types remain ACIP-recommended, regardless of the year of the vaccine or the individual yearly approval, as long as access is through the shared clinical decision-making guidelines, which could be how all COVID vaccines are accessed from this point forward.
It’s almost a better system, to be honest, as it allows for additional vaccines.
Also, please note that RFK Jr. did not establish this method. The previous administration set it up as a tool to protect access to these lifesaving vaccines.
While we should and will contact the House about Impeachment, we should also contact the Senate about both passing the ACIP bill and impeachment.
And although some think going state by state is a good plan, it’s certainly a viable approach, but it comes with a lot of risks… and more importantly…
Red states are on the list, and they are unlikely to go along with that strategy.
So, we should go to the source of the problem, and it’s not RFK Jr. for once.
CVS and Walgreens are setting limitations not required by any regulator.
That’s our first stop.
We should first contact CVS and Walgreens’ help lines and inform them that they are not following the current guidelines, nor are they allowed to require prescriptions for COVID-19 vaccines. While also making a huge mistake by not ordering Novavax.
We should also share this information with members of Congress so they can put pressure on CVS and Walgreens to distribute them properly. The same is true of State leaders who are being asked to write unnecessary E.O.s or public health orders.
This should still happen and will reduce liability, but red states will not comply.
If you want to go the extra mile, contact your state reps to confirm that access is allowed via the shared clinical decision-making guidelines without documentation.
That should immediately open up access.
Then we work with the HELP committee to try to get the meeting postponed.
At the same time, pressuring a combination of Congressional committees to initiate impeachment proceedings based on RFK Jr. continuously perjuring himself to Congress, which is likely to continue at today’s Senate hearing.
While simultaneously pushing through the bill to legalize and reinstate ACIP in the Senate, adding the reinstatement of the removed Senate-approved CDC Director.
All while you all are making public comments to the illegitimate ACIP.
We want to complete all this before these two workgroups can meet and further alter the recommendations. And it all starts with calling CVS and Walgreens, while ramping up for the continuous run of RFK Jr. committing crimes in Congress.
We should also use this time to push CVS and Walgreens to order Novavax.
In the past, Novavax had a short shelf life, resulting in significant waste.
With the expansion to six months and single-use vials, that problem is gone.
However, just like everything else, they don’t know if we won’t tell them.
So, now that you’ve seen the thought process, let’s break it down into something a little less complicated.
Fix pharmacy barriers at the corporate level:
Contact CVS & Walgreens to remove non-required limitations, considering that the ACIP recommendations have remained the same; access constraints have not been implemented at this time, and are unlikely to alter the shared guidelines.
CVS: 1-800-746-7287
Walgreens: 1-800-925-4733
Don’t forget to mention that they should order Novavax.
CVS is limiting access in the following states: CO, FL, GA, KY, LA, ME, NY, NC, PA, UT, VA, WV, MA, NV, MN, and DC.
Walgreens is limiting access in the following states: AZ, CO, GA, IN, LA, MO, MT, NM, NY, OR, SC, UT, VA, WA, WV, and WI.
The two groups, having different lists of states with limitations, clearly demonstrate that there is no rhyme or reason to this.
We will update numbers as we start finding new ones to call.
Lock in state-by-state access:
Contact your state health officer/board of pharmacy (and legislators) to confirm COVID vaccine access under shared clinical decision-making.
Use them to add pressure to the push at CVS and Walgreens.
The 21 states (and DC) in question are Arizona, Colorado, Florida, Georgia, Kentucky, Louisiana, Indiana, Maine, Missouri, New Mexico, New York, North Carolina, Pennsylvania, South Carolina, Utah, Virginia, West Virginia, Massachusetts, Nevada, Minnesota, Wisconsin, and DC.
Edit: 21 is down to 16 as of 9/8.
We may add them later, but for now, you’ll need to look it up.
Contact the Governor’s Office, the State Pharmacy Board, and the state’s public health leadership to inform them of the correct regulation in your state.
Flood the public record for ACIP:
Submit written and oral comments for the Sept 18–19 ACIP meeting.
ACIP public comment page: https://www.regulations.gov/commenton/CDC-2025-0454-0001 Public comment is open from 9/2/2025 to 9/13/2025 at midnight.
Emphasize the illegitimacy of this committee, as well as a pharmacist’s authority to order COVID vaccines, shared clinical decision making for access, and avoiding added gatekeeping that isn’t required by regulators (i.e., the same stuff you talked to your state legislators, state health officials, and corporate pharmacies about in steps 1 and 2).
Push for the recommendation to remain as wide as possible, so as not to overcomplicate access, while leaving the shared clinical decision-making guidelines intact.
Congressional oversight:
Hold RFK Jr. accountable for all the stupid things he says to Congress.
Advocate to push through the bill for Senate oversight of ACIP, including reinstating the previous ACIP members, and adding the reinstatement of the removed Senate-approved CDC Director.
Advocate to Congressional Committees and eventually the Judicial Committee to initiate impeachment proceedings of HHS Secretary RFK, with an eye on upcoming hearings where we anticipate him to continue perjuring himself.
Contacting the committee he’s meeting with on Thursday to lead RFK Jr. to explain how people will be able to get the vaccine.
Show how RFK doesn’t know where he is from meeting to meeting.
Be prepared for him to perjure himself. Don’t get caught slackjawed.
And most importantly, call CVS and Walgreens.
CVS: 1-800-746-7287
Walgreens: 1-800-925-4733
Thank you for taking the time to protect our public health.
Next Article: Is Novavax the Better COVID Vaccine?
If you are a new reader and want to follow up with some of my work…
Amidst this, I started doing a show multiple times a week in early 2023. We formed a group and consistently did the show to push successful direct action.
This led to presentations and direct contact with members for further action…
The COVID presentations employed an “inside/outside” strategy. We did the presentation “inside” the meeting, but also had the public contact from the “outside” with not only public comments but direct contact via academic emails to members.
If you are unclear, VRBPAC is a committee of the FDA and, with that, the HHS.
Our work has been cited in a few articles.
If you’d like to follow my social media or make a donation, the links are provided below.
Brace for Impact is on Twitter and X on Tuesdays and Thursdays at 6:00 pm PST.
You’re also welcome to join our Discord, but be prepared for a small test to enter.