Our Continued Success Requires Us Building on What's Worked...
And we have a lot more potential for success than folks realize.

This is my first article of 2024 and I really do owe the community more content. The Novavax timing article is coming up but I won’t lie, this IgG4 issue is confusing and poorly defined while exceptionally important…
But let’s be real, the only reason I even need to write that timing article at all is because of the outstanding work done by everyone who contacted the ACIP and VRBPAC committee members by writing them letters last year.
I’ll breakdown the Nova timing at the end but for now let’s focus on the task.
This article is going to try to show not only how we’ve won but how we can continue to win. (Spoilers: it’s by working together.)
A quick explanation is in order…
What are these groups?
ACIP stands for Advisory Committee on Immunization Practices and is a committee within the CDC.
VRBPAC for Vaccines and Related Biological Products Advisory Committee and is a committee within the FDA.
They are both advisory in nature to their respective groups. They work separately but also together to oversee vaccine regulatory decisions and we spent the greater part of a year finding ways to contact these members.
Contacting these groups culminated in a public comment turned presentation where after a few months all of our asks were met…
Some in ways we didn’t expect.

You can read that presentation here.
Some of their response came in what I would call abnormally shaped boxes but the outcome ultimately led to Novavax access being made widely available and clear guidance that allowed folks access to multiple shots with limited interference.
Folks w’re having to do all kinds of ridiculous things to restart a primary series and suddenly those road blocks were just gone…
Really an amazing outcome.
This effort even inspired other people and has rolled out into a few other groups trying to do similar actions and frankly, I welcome it.
Creating change when going against some of the most powerful forces takes a lot of work and the more the merrier is usually the way to go…
Sometimes those groups can even work together.
And working together has really paid off lately…
Recently we had a few big wins and at least one went under the radar…
First off, the Census was going to change how Disability was tracked for their process that would have dramatically reduced the amount of disability we are seeing in our communities and after immense public pressure they decided not to change the method for gathering that information.
Estimates had it undercounting the disabled population by half.

And second, we also had an unexpected win at HICPAC.
This was a CDC group that was changing regulations which portrayed surgical masks to have the same quality of protection as respirators.
With several airborne pathogens on the rise, I couldn’t make sense of this.
By the looks of it… no one could.
This was already clearly defined within their procedures but they were going to move forward with it regardless. This was not the product of one meeting, it had already been decided and this was a final vote.
We were a bit late but there was a big push from MANY GROUPS to not let them drive through what could only make sense as a cost saving maneuver.
For all intents and purposes this was a total victory.

The CDC even said they would push to have more experts in the correct fields as part of the already large committee… While there are just a handful of voting members the actual committee is quite large and there’s no excuse for not having those experts.
That being said, we all approached the problem very late in the game from an activist’s perspective and the expectation for success was very low.
But in the end, grassroots activism works… IF you can get enough people.
Now, while the Census situation goes in the “problem solved” pile, HICPAC is a different story. This is going to need constant pressure as the CDC is kicking this back to the committee because it didn’t meet standards of care.
But that’s not the only issue with standard of care at the moment…
The CDC is considering reducing COVID isolation.
There is a talk they might reduce it to a single day of isolation.
This is not happening in a vacuum; Oregon reduced the isolation back in May.
Their reasoning was not great.

And I know what you’re thinking, did Oregon see a big spike right after this?
And the answer is no… There was actually a small decrease which makes me think they altered the method of counting COVID hospitalizations.
I do know that around then they moved to tracking lab tested hospitalizations only, but I cannot confirm how that timing might have altered the data set.
I assume it would be favorable to minimizing arguments.
Feel free to leave a comment on what I might have missed there…
Regardless of how, they created the data points they wanted and now California recently made the same move to limit COVID isolation to 1 day.
This is the dominoes falling on “getting back to normal” where COVID is not significantly interfering with daily life, but they just mean for corporate profits.
Unfortunately for them, if we want to get to a place where COVID isn’t actually interfering with our daily life then denial isn’t the best strategy.
Our Public Health leaders are capitulating to their corporate bosses, so that the “burden” of COVID is carried by the people instead of their profits.
But really, if they actually competently cared about profits then they would be taking a different track where they protect workers and create a safer environment for all.

Let’s call this what it is…
A complete removal of COVID isolation altogether.
Luckily, that’s not the end of the story.
We’re gonna get lucky here because the release was immediately met with fierce opposition and in some reports it’s already being called “preliminary.”
On, a side note… You can see that by reducing the isolation to 5 days, which is not enough, made it so that minmizers could claim that it wasn’t helping stop the spread, simply because it’s not enough time.

This is similar to the mask reviews that had healthcare workers only wearing respirators for the time they were at work while claiming spread at home proved they didn’t work at all because they were still infected.
In this case though, the final word on this matters a lot…

Because that means this is not a done deal, and we should offer the CDC director our free “consultation” services…
We do that by making our voice heard.
So, light up those phones.
Call them daily and leave a message…
The old system for leaving comments via phone message is still intact; it might take a second to get the right person but we’ve already heard of it being an option.
Be polite, but stern.
Here are your contacts… This is not a done deal.
General CDC phone number: 800-CDC-INFO (800-232-4636)
TTY 888-232-4348
CDC Director’s email address MandyCohen@cdc.gov
CDC Director’s phone number: 404-639-7000 (press 8)
CDC Director’s address 1600 Clifton Road Atlanta, GA 30329
CDC Director’s fax number 404-639-7150
And if you feel up to it also contact California and Oregon Public Health too.
Now we circle back around to ACIP and VRBPAC.
Remember, these committees happen every year… multiple times a year.
ACIP: Laying out a vision
This is on Feb 28th and as of writing this article there are 8 days to comment.
The name says it all… Advisory Committee on Immunization Practices.
These folks deal with any type of vaccine practices for the CDC.

Wednesday, February 28, 2024
8:30am EST - COVID-19 Vaccines • Introduction Dr. Matt Daley (ACIP, WG Chair)
COVID-19-associated hospitalizations among adults - COVID-NET Dr. Christopher Taylor (CDC/NCIRD)
COVID-19 vaccination coverage update Dr. Kevin Chatham-Stephens (CDC/NCIRD)
COVID-19 vaccine effectiveness Dr. Ruth Link-Gelles (CDC/NCIRD)
Economic analysis of an additional dose of COVID-19 vaccine Dr. Lisa Prosser (University of Michigan)
Evidence to Recommendations or Work Group Considerations Dr. Megan Wallace (CDC/NCIRD)
Next steps for the COVID-19 vaccine program Dr. Lakshmi Panagiotakopoulos (CDC/NCIRD)
1:35pm EST - Public Comment 1:55pm EST - VOTES • COVID-19 Vaccines Dr. Megan Wallace (CDC/NCIRD)
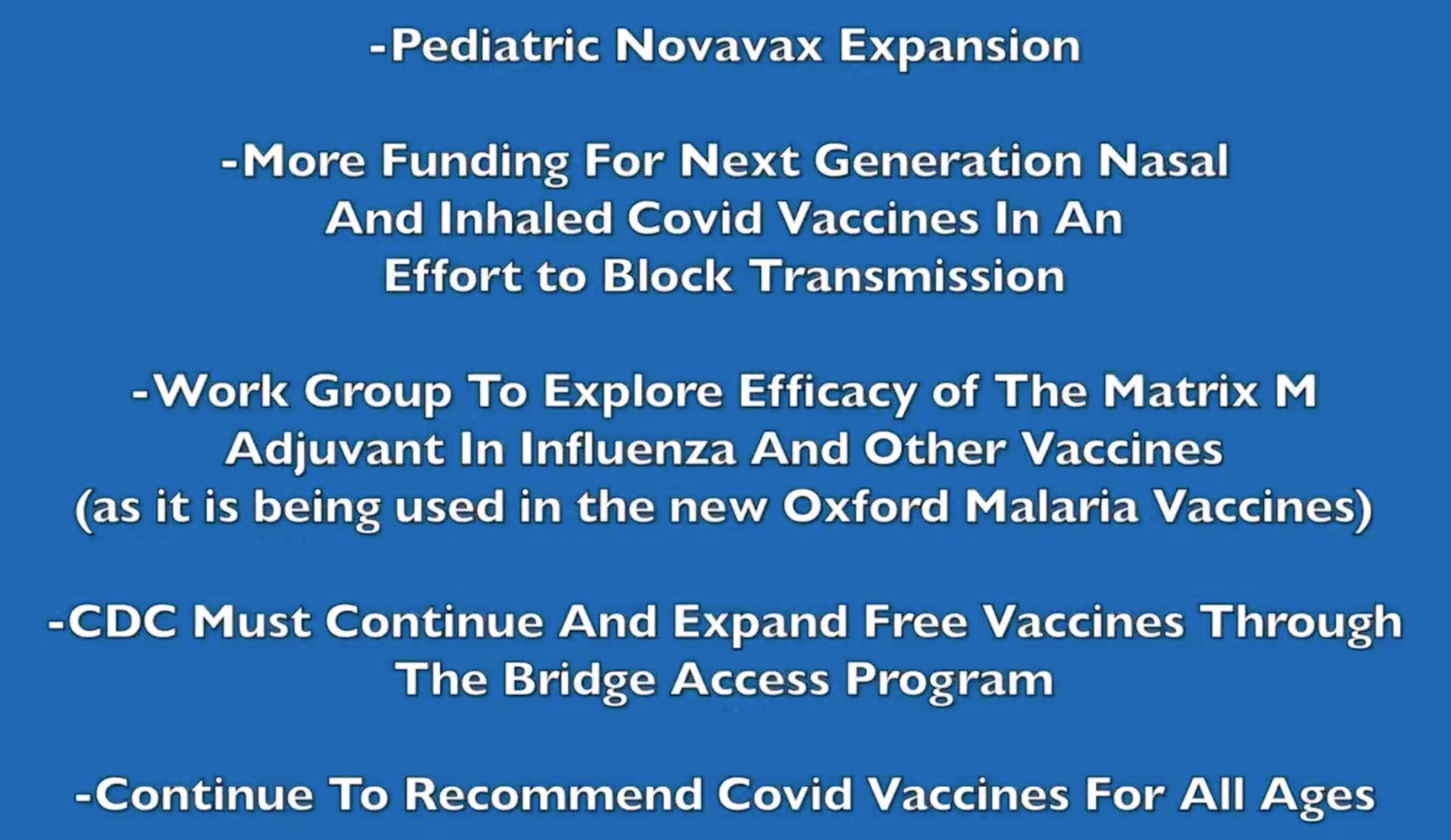
Now for both ACIP and VRBPAC, we want to lay out a larger agenda…
- Work Groups to explore Matrix M as an adjuvant for flu vaccines and see if it can improve efficacy in the same way that it did for the Oxford vaccine.
- Novavax expansion of usage for pediatric use. Novavax for children is the EXACT same vaccine and dosage, so the vaccine your kids need is already going to waste but they simply cannot access it. There is no reason that it can’t be expedited instead of waiting for the normal fall approvals.
- COVID vaccines must continue to be recommended for all ages, with vaccines made available to anyone every six months.
- More funding and Work Groups for “Nextgen” nasal COVID vaccines.
- CDC should continue AND EXPAND the free vaccine Bridge program.
Leave a comment here, there were around 900 at the time of posting.
VRBPAC: What to expect
Vaccines and Related Biological Products Advisory Committee.
This committee hearing will be March 5, 2024, at 9 a.m. EST.
With 19 days as of Feb 14th to still write a letter.
“This meeting will be held to discuss and make recommendations on the selection of strains to be included in the influenza virus vaccines for the 2024 to 2025 influenza season. The meeting will be open to the public.”
The big deal here will be pushing to integrate Matrix-M with the Influenza shot.
You are more than welcome to list off all the other elements proposed for the ACIP meeting but this meeting appears to be focused most specifically on the Flu vaccine…
That being said, it doesn’t hurt to say it anyway.
And there is one more thing…
There is one additional thing that can done be with the FDA and that’s partnering with an HHS division called The Administration for Strategic Preparedness & Response who oversees access to Monoclonal Antibodies and other existing antiviral COVID treatments.
I think I have that group right but it can be shortened to HHS to be safe… and this partnering would be done to study repurposing existing mABS and other infusion treatments for usage against Chronic COVID infections.
It’s becoming increasingly apparent that the Chronic condition that is Long COVID shares mechanics with the Acute phase and that means existing treatments may help lift the burden of Long COVID by treating persistent virus in degenerating patients.
This is already being tested in the UK as well as other countries. We can’t be left behind on this and we need to pressure the FDA to act regarding reapproving existing infusion treatments for the purpose of trials to stop the degenerative effects of LC.
The persistent infections simply need to be matched to infusion treatments that we know would have worked around the time the person was infected.
It’s a long shot, but the science backing it is growing in volume.
You can leave a comment for VRBPAC here.
Jesse and Paulie have been crucial in helping lead these actions, give them a follow.
We also have ‘Brace for Impact’ on Tues and Thurs.
That’s Tuesdays and Thursdays at 5:30 PM Pacific with some more stuff coming up.
Thurs Feb 15th —→ SPACES RSVP.
Missed it? You can follow our new Twitter account for the show here.
Also, our Discord is thriving so if you feel like you need that community drop on by and check it out, this invite is good for a week.
Feel free to ask for a new one in the comments.
If you appreciate my work consider subscribing or making a donation via Paypal, with the latter being the preferred method of support.
But I appreciate the support from everyone in any form, so give this a share and let’s make things a little better.
If you want you can find any of my socials at my linktree.
But let’s be real you didn’t read to the end for all that…
Novavax Timing explained… no sources.
Nova timing is 2 shots 2 months apart with a 3rd 6 months after the 2nd.
That’s 3 in 8 months total.
You maintain this with a shot every 6-8 months.
You can get a booster or update either 2 months later or you have to wait the full 6 months but you only need one update if you maintained the response.
No new vaccines, of any type, during that period from 3-6 months post.
That’s the pesky IgG4 issue and it’s a doozy.
If you already got an mRNA update then you can get a 2nd shot at 2 months but you still have to get a new primary series 6 months later for the full Matrix-M response.
So, it’s up to you how you want to handle that and since everyone is going to ask, you’ll have to wait on sources for all that until next time.
Hopefully it won’t be too long.
In the meantime, let’s try to find new ways to work together instead working against each other.
If we share the same interests then we should be able to prove it.
Thanks Don! Love the positive message of hope n encouragement and ways to continue to advocate. :-)
Thank you Don