

The Risk of Long COVID Explained.
We need to be clearer about the risk associated with any infection.

This is ‘The People's Strategist.’ A newsletter dedicated to Strategy for all things related to the People. Right now, that’s all about making sure you have the information to keep you and your family as safe as possible in these troubling times.
The goal here is to answer folks’ questions about COVID strategy based on risk.
And as protections from COVID are being removed, they were often called “mitigations” or “mandates” but they were protections… Folks have a lot of questions.
The most common questions I’ve seen asked among so many related to COVID is…
What is the risk of becoming a long hauler from an infection?
And what is the risk from multiple infections?
I’m going to cover these two questions in great detail, but first, it will require explaining a few things to make sure we are all on the same page.
If you are opening this article, you came for one of three reasons…
1. Morbid curiosity.
2. You are concerned about the risk to you or your child.
3. You came to diminish the nature of the risk.
The thing is that this affects us all equally, so if you came to troll… This affects you too.
This is my first substack article but I had previously published an article about the risk associated with our situation last October on Medium.
Many, if not all, of my theories or concerns came true.
If I at least pique your curiosity, give me a follow, and you’ll be sure to see the next parts… and I have a ton of material to cover. Throw a comment to let me know what you’d like to have explained, eventually, I’ll start taking political questions too.
And please, more than anything… If this resonates, SHARE this article.
The information is useless if only a few people know it.
(Update: Since I’ve fielded this question a bunch, everything that is underlined is a source. If you feel that something could be sourced better or is missing one… Leave a comment and I will address or fix it. This article is being regularly updated.
2nd Update: After 38.3k views, a reader found out I’m doing this alone and it has been full-time for over a year so they insisted I include a donate button… Paypal.)
But right now… Let’s stay focused, we have a lot of ground to cover.
We’re just talking about the risk of Long COVID and a lot of numbers have been batted around. There are more than a few complicated variables that need to be understood before we can create a complete idea of the actual risk.
The Pretext is that SARS-CoV-2 is the virus, and COVID-19 is the disease.
I will refer to it generally as “COVID” but understanding the difference matters.
First, let’s start with what is Long COVID?
Long COVID is not a single ailment. It's a combination of a variety of symptoms that cannot be explained in any other way but from a COVID infection. It can be caused by an acute infection, asymptomatic infection alone, or appear months after the infection.
The WHO also classifies it as “persistence of symptoms beyond 3 months of SARS-CoV-2 infection, lasting for at least 2 months and not explained by any other illness.”
And many folks who get it will never even know they had an infection.
Folks who suffer from any combination of symptoms are known as Long-Haulers.
The disease would be most encompassed by calling it “Long COVID Syndrome.”
It can be defined as damage from infection, persistent virus, or autoimmune attacks.
All of which have entirely different scales of both damage and healing. Symptoms could include just one or all three, each experience is unique and none are trivial.
It’s important to distinguish that the name ‘Long COVID’ is a bit deceptive in that it makes folks think it’s simply the COVID acute infection period stretching out longer but that’s not entirely accurate as it’s not the whole picture.
This is why there has been a conversation about giving it a more official name, but these terms serve to limit who can be included when it needs to be totally inclusive.
Why?
Yes, these symptoms can obviously spring up during infection and never go away but also, they can appear months later as your body tries to heal. So, if you were an asymptomatic case, you could easily fall between the cracks and not get help.
And it’s not just that part that’s confusing…
It is a combination of what can seem like a random assortment of symptoms but some are more common than others and there is some or no correlation between them.
Two people could have similar symptoms for totally different reasons.
This can include but is not limited to neurological, organ, vascular, & reproductive damage. It can be caused by lingering virus and damage from viral syncytia AND what appears to be your body trying to heal from it...
But really, they are all the same thing. Those are the stages of a COVID infection.
When we say COVID is neurological, it means COVID damages our body’s ability to send signals, and as our body is a massive fine-tuned conduit for all the things that make it run… Altering these signal pathways can have very negative outcomes.
But how does COVID do this?
It’s all damage from the creation and activity of ‘viral syncytia.’
Because at their core, both SARS and COVID are “Syncytial Viruses.”
Others are HIV, Herpes, and RSV…
Even MERS did this.
I should point out that all of those listed are known to have similar mechanisms.
This process includes removing your cells from their natural positions.
And that stops your body from sending signals properly.
It can do this all over your body.

It’s important to distinguish that the distinction in the media between “mild” and “severe” is about whether COVID can do this process in your lungs.
Omicron, or BA.1, was considered “mild” because it didn’t do this as well in our lungs.

That was actually the only thing they even checked before declaring it mild.
Even though Omicron was responsible for more deaths than Delta and a third of all pediatric deaths happened in that time, for some reason… This is our defining metric.
And let’s not forget that Omicron can still make syncytia just fine in other places.
Plus, the next oncoming dominant variant, BA.2, creates syncytia in the lungs again.
There is a handy chart toward the end to help with visualized comparison.
There is even a second variant called BA2.2 that is destroying Hong Kong and since originally writing this close to a dozen new variants have shown their ugly head.
The further we let this go unchecked, the worse it will get.
BA.2 is believed to be 1.4x as infectious as its predecessor and it’s important to say that we’ve seen this demonstrated. Expect each variant to continue on this track.

But it’s SOOOO important to say…
ALL the COVID variants have been doing this damage all over our entire body.
This is the problem with thinking of it as a Respiratory Virus alone. It creates this image that the damage is limited to your lungs, but the damage is in your entire body.
That’s one of the reasons why Long-Hauler symptoms can seem so chaotic.
A study was done in 2020, it estimated that there were more viral particles during peak infection than cells in your body. It was actually thought to be 10 to 1.

That’s between 1 and 100 billion viral particles, and this was in the early stages.
Being infected with a virus is best comparable to a house infested with termites.
Because of this… You have to understand that COVID is all over your body.
Consequently, it’s much better to think of COVID as a Vascular Disease caused by SARS-CoV2 that triggers a complex series of auto-immune attacks, extracellular dysfunction, cellular apoptosis, and death; and there is no pill for any of that.
While the truth is closer to a “Respiratory transmitted virus that causes disease, dysfunction, and death to every type of cell in your body.” But that’s a bit much.
It breaks down like this…
Your body has four types of tissue; epithelial, connective, nervous, and muscular.
COVID can cause dysfunction or cell death, or apoptosis, in any type of cell group.
It can even create an AIDS-like syndrome where your T cells stop functioning.
(More on this in a future update.)
But most folks don’t have a great conceptualization of what “Everything” means…
So, we will use Vascular Disease for visualization… Everything your blood touches.
The actual damage though happens in two parts…
One part is during acute infection, which you can see above.
That chart demonstrates that it takes about five hours for COVID to start forming syncytia and invade your body.
So, that’s your window for action post-exposure…
Though I don’t suggest playing that game.
Omicron has likely sped up this process.
To give you an even better idea of why I don’t suggest you gamble it is because this is COVID in your Olfactory Nerve…
Which is, for practical purposes, PART of your brain.
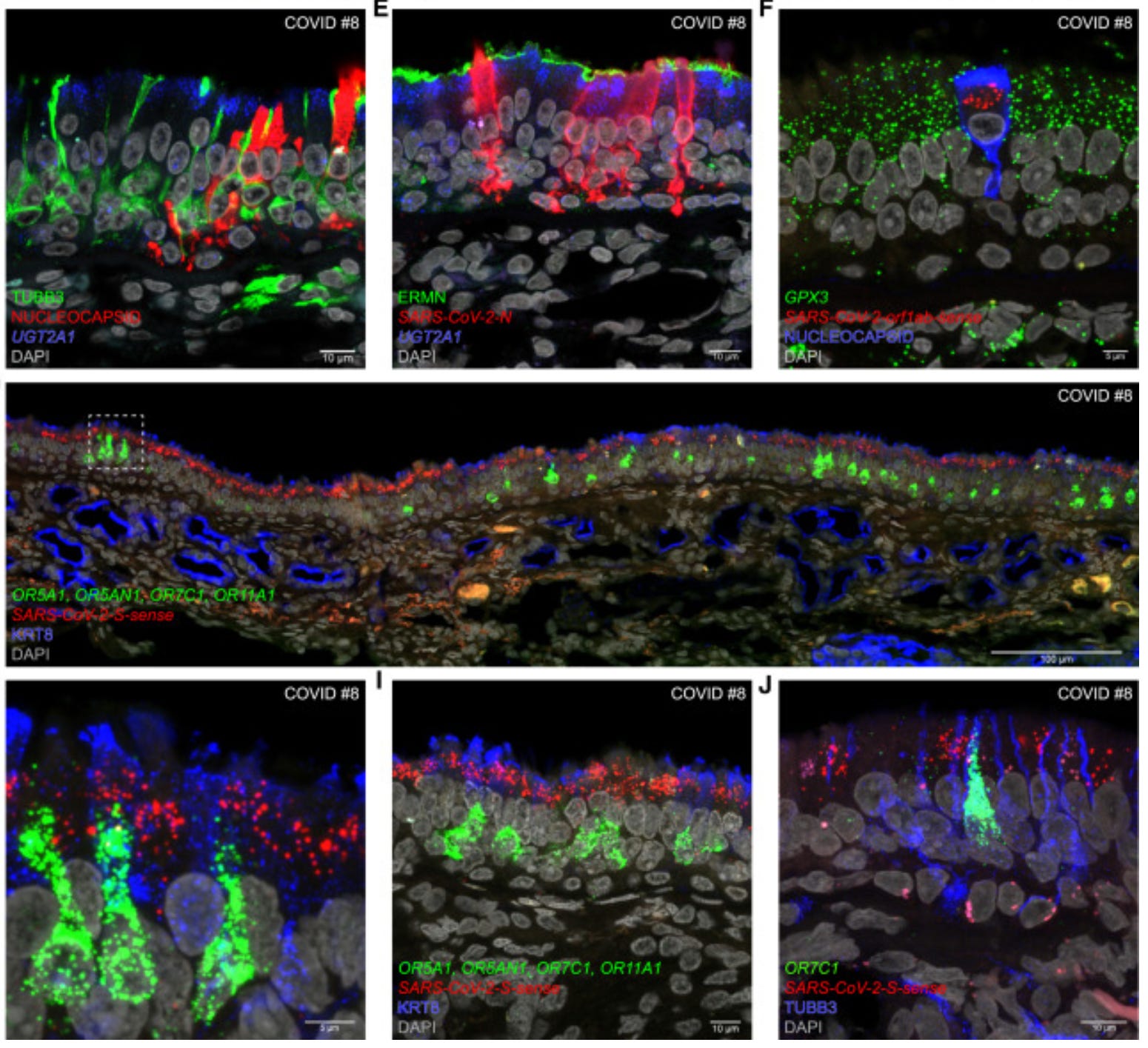
COVID doesn’t always act in a biologically linear way as we think of it, the study these photos are from explains that COVID gets in your brain directly via the Olfactory but it skips the bulb and instead enters the larger part of your brain.
Before that “SARS-CoV-2 can enter the nervous system by crossing the neural–mucosal interface in olfactory mucosa, exploiting the close vicinity of olfactory mucosal, endothelial and nervous tissue, including delicate olfactory and sensory nerve endings.”
Folks need to understand how little ground it has to cover to get into your brain.
Basically, once it’s in your Olfactory… That’s your brain.
There is no Blood-Brain Barrier to protect you when COVID is riding in your cells.
And the only protection is the mucosae, a tiny thin layer of skin that is LOADED with access points and even Omicron has no problem exploiting this entrance.
It is literally a mucus membrane. They aren’t notoriously durable against pathogens.
Anyone who says “we don’t know if COVID damages brain cells directly” is wrong.

Considering how Airborne transmission works, we are extremely vulnerable.
It’s kind of shocking that we’ve been so blasé about air quality this entire time.
When we finally do what is necessary to stop COVID, we will kill a few viruses.
But here is why I’ll be wearing a mask even after we exterminate COVID.

The real important thing is that no matter if the particles are dispersed close to you or far away they reach a constant point where they linger in the air for hours.

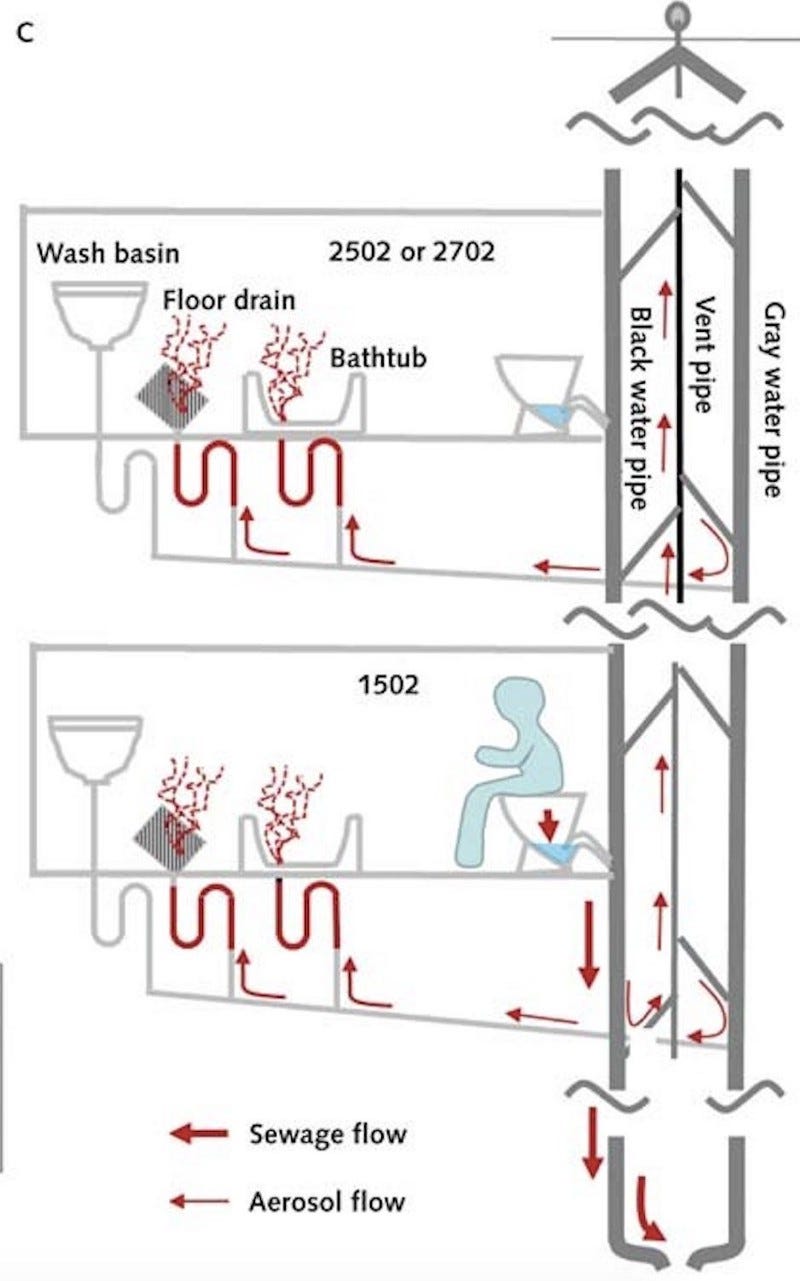
You can even pick up the virus if an infected person had been in an enclosed space with poor ventilation hours after them like a shared bathroom in that example.
Or if ventilation is shared…
There are even examples of vertically attached bathrooms spreading COVID when you flush the toilet. It’s known as “fecal aerosol transmission.”
Here’s how it works… Western Style plumbing might avoid this.
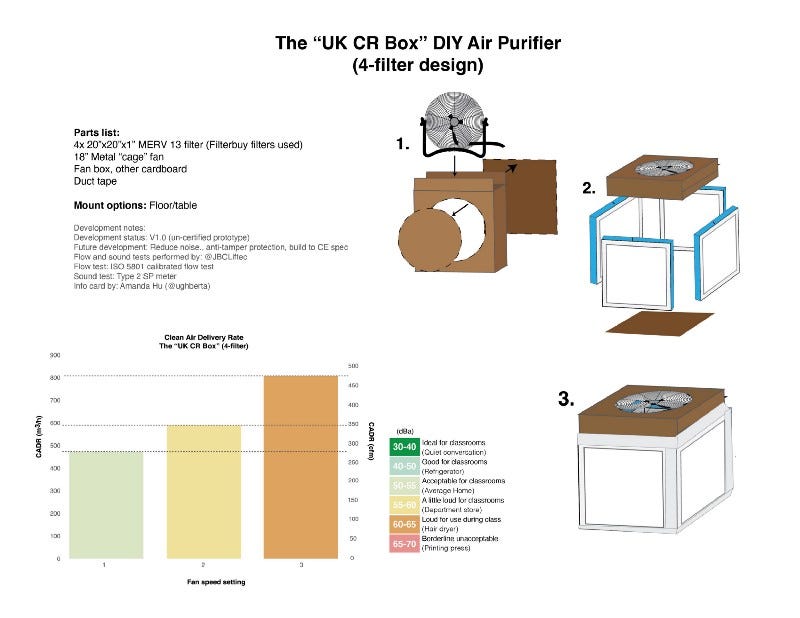
The annoying fact is that … any HEPA air filter will catch COVID, so even minimal effort will go VERY far.
And there are multiple examples of Schools and Gyms staying COVID-free by focusing strictly on Air Filtration. So, this isn’t impossible.
If you want to get really serious, it looks something like this…

If that’s too much, build one of these… They are already popular and well tested.
The can be done relatively inexpensively and last for a significant amount of time.
And just so everyone can quickly understand the difference between ventilation, filtration, disinfection, and doing nothing…

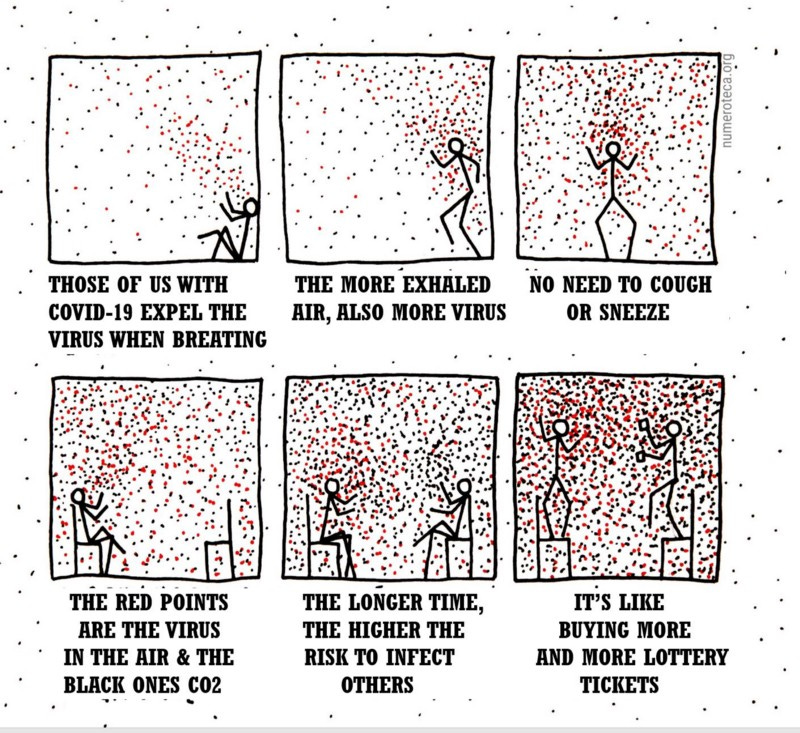
But what are we going through all this effort for?
See those dots? Those are micro aerosols and droplets containing COVID.
Here is a model of what those delicious micro aerosol droplets look like…
Even if that didn’t have COVID in it… That’s quite literally ‘Lung Juice.’

It’s important to note that a recent study showed us that a single virion, a viral particle, the purple cell in the photo, was enough to begin an infection.
That study went on to say…

This was the first controlled and studied infection to date. I want to point out I have very mixed feelings about the ethical nature of this study. But the data is clear…
Regardless of the severity of symptoms, asymptomatic or not, the risk of infection is the same if an infected person won’t wear a mask… And not just any mask.
There has been some debate on the validity of masks when a virus is so infectious.
Though infectiousness doesn’t alter the physics, just increases this risk.
But just in case, here is an article with 49 studies showing masks work.
But for some people that won’t be enough, so I am going to explain it.
This is a photograph of COVID occupying a cell where it will do what is known as “parasite” the cell and seize control of its mechanisms.
COVID and all Viruses are classified as ‘Obligate Intracellular Parasites.’
Because they cannot reproduce or replicate outside of a host cell.
Why anyone would willingly make themselves a host to something like this is beyond me, while Urgency for Normal is acting like our bodies are a COVID BnB.
Once folks understand this better there will be a greater push to clean indoor air.

Now, if you notice that picture shows that a COVID virion is approximately 100 nanometers. But if you understand Micro Aerosols, I propose the name Microsols, but it doesn’t matter… then you know that COVID “rides” in lung fluid as shown in the picture just above this one… Those lung fluids are approximately three times larger.
That means a liquid micro aerosol is approximately 300+ nanometers.
300 nanometers is .3 micrometers or microns.
An N-95 will handle anything above .3 microns.
The micro aerosol COVID rides in are slightly larger than that.

So, an N-95 or a Chinese-made Kn-95 is the MINIMUM protection to stop COVID.
But the Chinese made can be unreliable if it’s from a random source.
Having learned this from personal experience.
Now, it’s critical to point out that ANY disruption of that fluid aerosol will significantly disrupt COVID because it creates the necessary environment.
COVID is VERY fragile but if you ignore this risk… And refuse to mask.
You will get infected.
Once COVID is in, and it will get in, it specifically uses something called sustentacular cells. This can get so bad, they hypothesize the loss of smell and taste is because the actual supportive cells are so damaged they can’t send signals anymore.
These cells are found in a few places in our bodies. Besides the nose, they are found in the testes and ovaries. This is probably why we are seeing a lot of damage to COVID patient’s testes… and it’s really bad. It even causes erectile dysfunction.
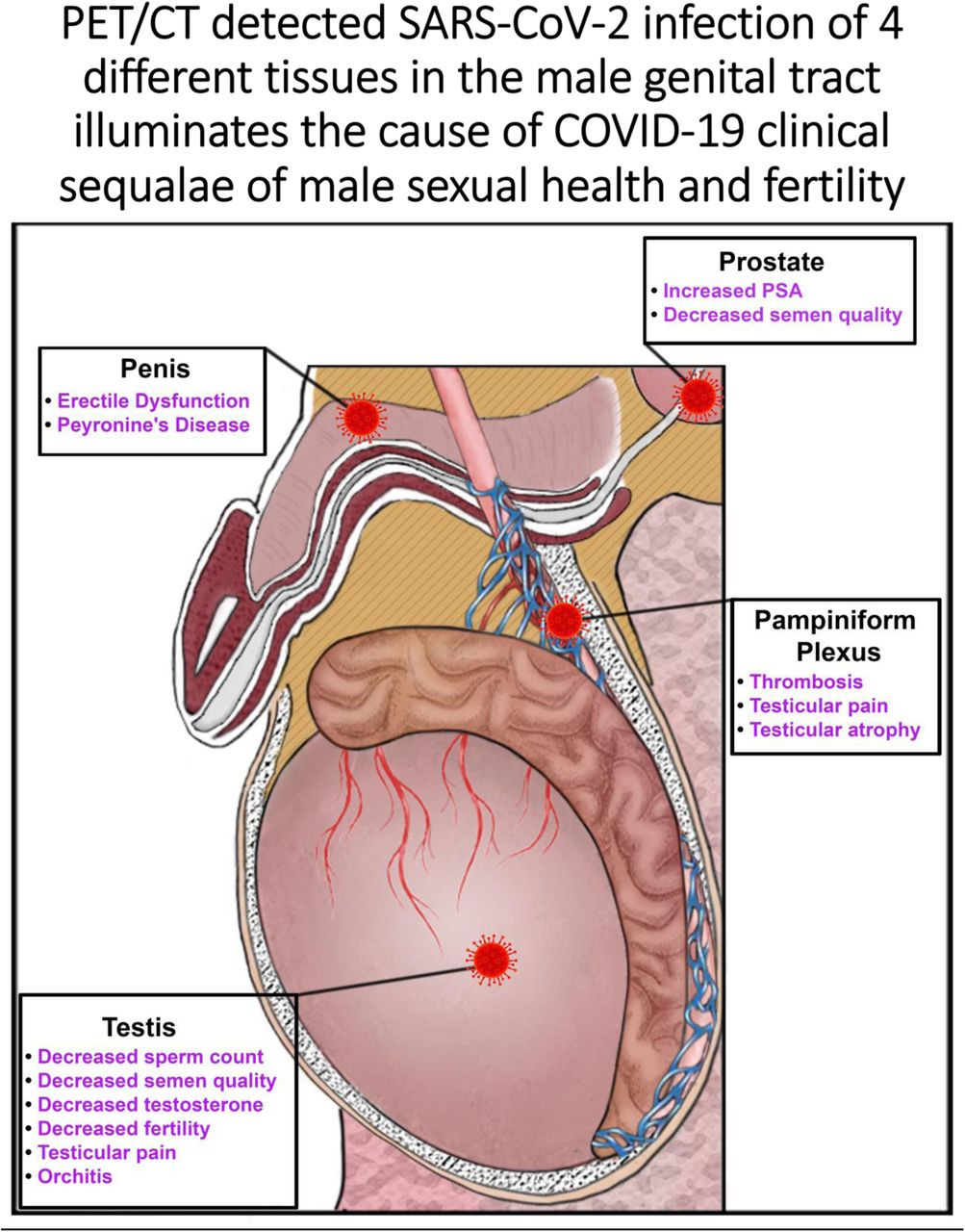
The additional viral reservoir might actually contain the virus and could be why folks without testes are more likely to have worse long sequelae like ME/CFS, but I digress.
Here is one more look at the differences between COVID infected testes and a control.
Control is on the left, but for the infected… “Asterisks denote high deposition of glycoproteins in the basement membrane and surrounding blood vessels.”
Don’t understand? The pictures give you the general idea that it’s not good.
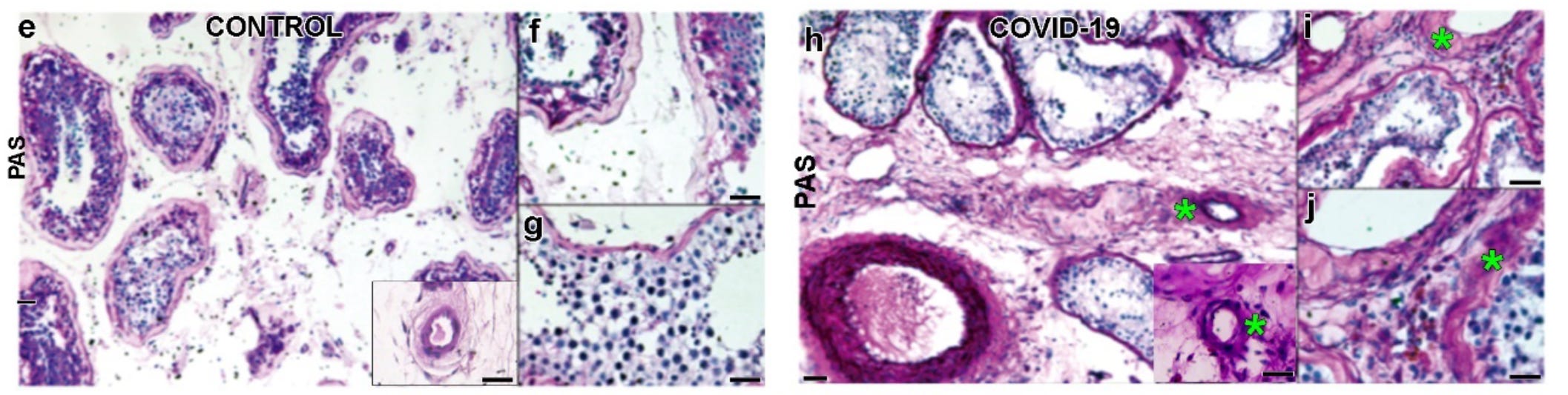
I’m still unclear, and maybe someone can explain this in the comments, why so many men are in such a rush to have their testes look like the picture on the right?
The truth is that all the folks who think that COVID isn’t a big deal…
Are going to end up with a “little deal” if you get my drift.
There is no amount of toughness or manliness that will protect from this.
The only guaranteed protection from this damage is wearing a properly fitting mask.
So, back to COVID infecting our upper respiratory tract.
Now at this point, you are still 2 days from having symptoms. So that’s two days of COVID doing its work, which goes like this… “SARS-CoV-2 appears to follow neuroanatomical structures, penetrating defined neuroanatomical areas including the primary respiratory and cardiovascular control center in the medulla oblongata.”
Here are pictures of it persisting in the Cerebellum.
It is incredibly difficult to clear the virus from here.

This leads to it attacking your autonomic functions, which are all the automatic functions of your body, and can lead to devastating consequences. It can even cause a specific type of stroke that is growing more common called a Cerebellar Stroke.
This is also next to your brainstem which is like a junction box for your whole body.
From there the virus can traverse your body in a few different ways.
All of them are bad.
Keep in mind that this means COVID is working its way through our brains front to back. It’s taking the scenic route through the material we store our memories in.
Omicron does this initial process quicker, which means it gets to replicating faster which is why the incubation rate has shortened, also known as part of the “Serial Intervals” which is the “time from illness onset in the primary case to illness onset in the secondary case.”
If the incubation rate decreases it’s almost certain the Serial Interval does too. That means more people being infected faster and more opportunities for mutation.

I’m going to add more to this and explain how this progresses in greater detail.
But for now…
Let’s talk about what happens post-acute infection.
The other part of infection is post-acute infection when the viral syncytia are still active but we might not have symptoms and our immune system starts reacting, both causing a variety of new problems we call “auto-immune” attacks… But both are caused by the same activity which encompasses a whole series of complex interactions.
It’s our inevitable biological reaction and our own cell’s ability to damage and invade its neighboring cells that really change the situation and rarely for the better.
This chart is not perfect, but it helps to visualize the general situation and concept.

Both of that combo can each alone trigger symptoms well after the acute infection and to be clear viral proliferation can continue deep into the Thrombosis phase.
As COVID hides in our own cells, it can get into cellular systems that are known as viral reservoirs. These can hide COVID for long periods, where it can reactivate.
This is often called “Persistent Virus.”
Then as your body tries to ‘rewire’ the damage done by the virus…
It can get very chaotic.
I think it’s a bit understated how much actual physical damage COVID is doing to your cells when you are a host to it. The process is extremely violent.
Imagine the worst house party ever… but in your organs.
On that note, if anyone says Long COVID is a simple issue, they are lying to you.
COVID does things that are abnormal beyond increased transmissibility.
COVID does its damage by creating viral syncytia, though its bursting has issues too.
But this all means that COVID does not have to leave a cell to infect the next, and that means our immune system has a ton of trouble fighting it.
The original SARS also created viral syncytia but it was poorly studied.
Keep in mind, SARS only infected around 8,500 people.
(Also the reason everyone in charge keeps acting like it’s going to just go away.)
But even then, it too caused a Long-SARS illness that left similar effects, and that linked study was based on a FIFTEEN-YEAR follow-up.
Doctors and scientists are extremely slow on the uptake of the importance of this. There is almost no one on Social Media talking about the syncytia nature of the virus.
It’s pretty much the most important and most overlooked element when talking about the risk of Long COVID. Because this is the process COVID uses to damage cells.
Here is an excerpt from an article about COVID’s infection process.
Even in this article, they claim SARS did not make Syncytia… But we know it did.

Creating viral syncytia not only helps it avoid our immune system, but it’s also part of the virus’s replication process.
It was not overstating it when I called it a ‘violent’ process.
More on that later…
Talking about Long-Hauler Symptoms.
Next, it must be said that a study from last year that claimed 80% of infected will gain AT LEAST one Long COVID symptom of the fifty possible symptoms they had identified, recently passed peer review…
Since that was released over 100 possible symptoms have been identified.
The original 50 symptoms broke down like this…

80% of ALL INFECTIONS will get at least one of these with quite a few added since.
This has become such a common issue, that hiring firms are warning employers about the implications of the American Disability Act on new hires. They make it very clear that many employees might not even know they are suffering symptoms.
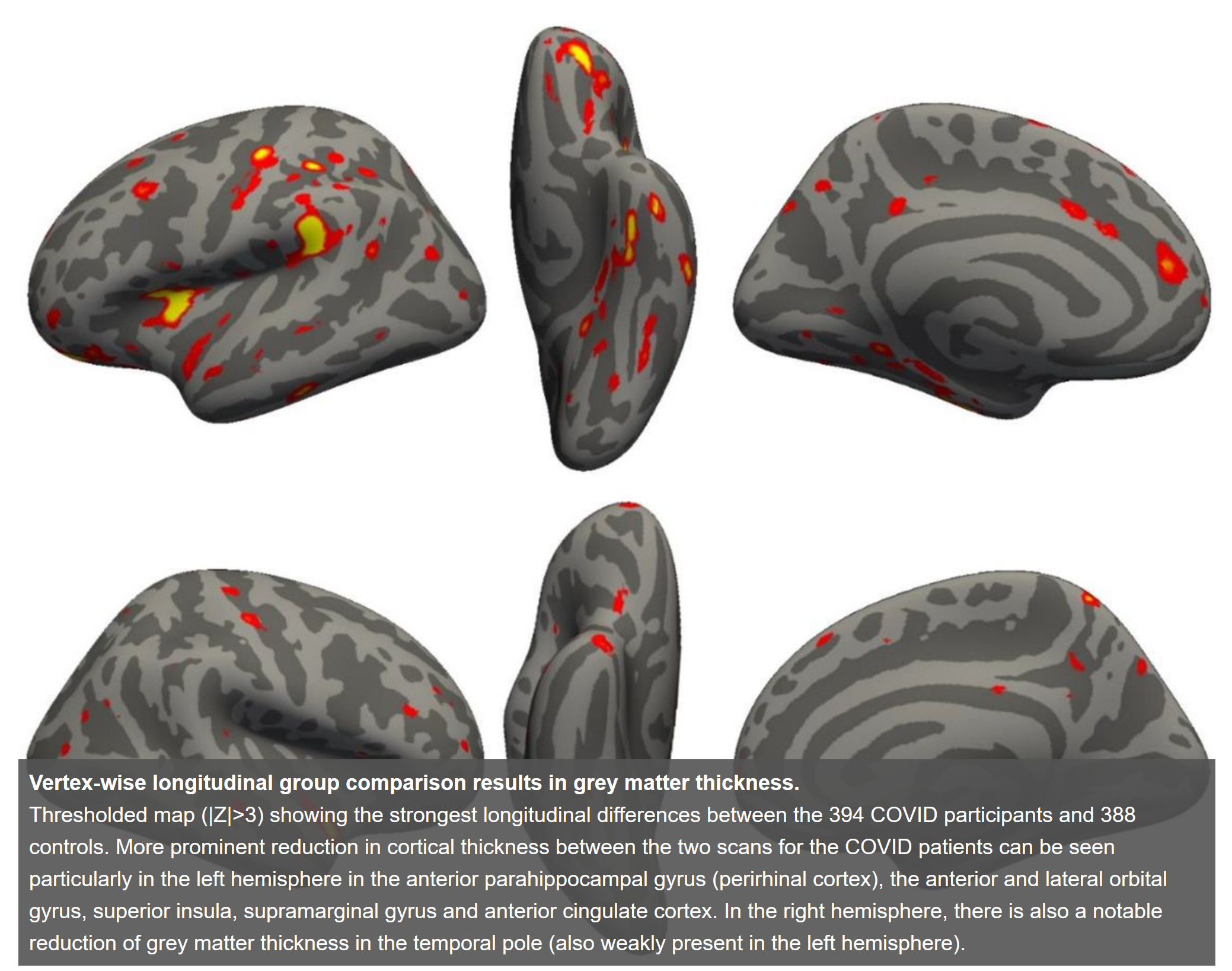
This is because the damage to our brain is very serious but that’s just the beginning.
This entire study was for detecting brain damage in “mild” cases.
This is the mild everyone is so excited about.
Our hearts are under equal or greater attack. Our understanding of the Long Damage to our hearts has grown a considerable amount in a short amount of time.

As you can see… This is basically like getting the worst superpower ever.
But instead of laser eyes or flight, you’re tired all the time and your hair falls out.
Heart disease risk goes through the ceiling… Destroys the Placenta and causes stillborn births… Studies are even coming out showing Kidney Damage.
Even the lungs, were only barely grasping the damage even in “mild” cases.
All of the yellow in this picture below is lung damage. Now, this was severe and fatal.

It just goes on and on with a new study full of horrors every day.
I personally had COVID in March of 2020 and even did a few interviews at the time while I was sick.
My experience was primarily digestive and it still took me 16 months to finally get rid of my digestive issues. I’ll explain what I did at the end of the article.
The important factor is that it took 16 months to feel like myself again.
Studies that used international cohorts have shown that recovery is very slow.
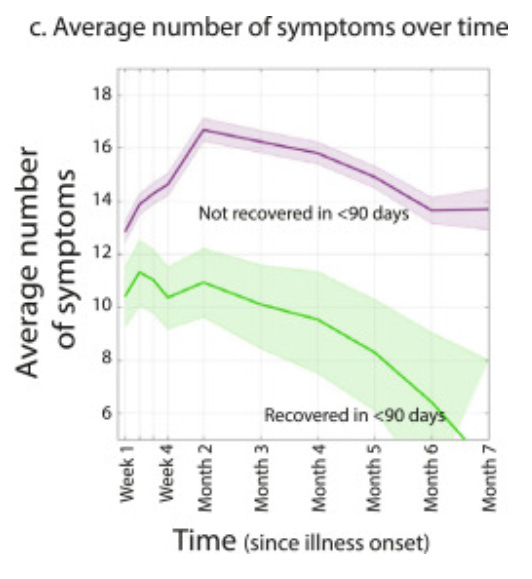
The chart is not my favorite to read, but it shows… more symptoms, more problems.
The greater number of symptoms, the less likely a full recovery is.
A recent study shows that a year later many were still suffering new heart conditions.
For me, I couldn’t Livestream, I was irritable, I couldn’t eat a ton of things, but still, I did not consider myself a “long hauler” because I thought I only had one symptom and not a combination of symptoms.
It turns out that not knowing you have Long COVID is a symptom of long COVID.

It should be noted that I was not great about treating my symptom and only managed to clear them somewhat accidentally. I probably could have done it faster had I tried.
Once my digestive symptom was gone, I noticed the irregular brain fog went with it.
I didn’t even realize it had been there until it was absent.
Many are having or will have the same experience.
But let’s talk about risk.
A lot of numbers have been batted around… Israel said last year that the risk to kids was confirmed at 11% but the number was likely higher because many children are nonverbal(<5) and are not great at explaining symptoms…
So, the risk was thought to likely be double that.
This was also back before tons of kids were getting infected in larger numbers with worse outcomes and before Omicron moved into the upper respiratory tract.
It was determined fairly early on that regardless of the development of symptoms, unvaccinated children have long been the primary driver of the pandemic via at-home spread as children make better viral reservoirs than adults.

This is probably why pediatric cases have skyrocketed since Omicron made its upper respiratory tract shift…. But this information is not even relatively new.
That data was from July 30th, 2020, so we’ve known this the whole time but the language was pretty weak when it came to explaining our risk.
Recent studies have been more … Aggressive with their language.

Call me a conspiracy theorist, but it really seems like contact tracing was canned simply because it consistently proved that children, whom we were told were not as badly affected by COVID, were at the center of the spread in western countries.
And even if they don’t develop symptoms, the risk is still the same…
Both for risk of transmission AND risk of Long COVID.
There is even a limited connection between symptom duration and risk.
Because the viral load is still high and damage is being done.

I will explain later that severity of symptoms is not the driving factor for Long COVID.
So, these kids are possibly even at GREATER risk.
And that risk is continuing to grow with each new more virulent variant.

So, even if kids don’t develop symptoms, which they are now, they can still spread COVID to their families at home, and the risk of Long COVID comes with that.
And there are plenty of studies that show the greatest risk of transmission comes from children who can then easily infect the whole family.
If this seems like an issue, it’s only the start of our problems
It’s becoming increasingly apparent that whoever said that kids were not affected by COVID was NOT an expert. Pediatricians are seeing the Long COVID cases now.
Hospitals are also starting to talk about a massive increase in pediatric admissions.

Expect this to increase, which means more kids with Long COVID.
(Update: CDC has released new data on pediatric hospitalizations… This is the danger of saying COVID doesn’t affect kids negatively in one chart.

Christmas was a super spreader event and our children paid the price.
I’ll never forget the White House telling us it was safe to visit family if they were vaccinated. There was still a risk of transmission and we can see the outcome.
Here is another way to look at it…

1400 kids have died from COVID since the pandemic started…
And half of them died since we made this change in strategy.
Because we started telling folks it was safe again around Halloween.
2nd Update: The CDC is attempting to revise its total pediatric death count by using a different system similar to what the UK has done to reduce COVID death numbers.
Basically, if a patient is a certain amount of time beyond their last testing date, they will remove COVID as a cause of death. To be clear, this is a repulsive tactic to make up for an improper response that put an entire generation at risk.
Families are without their children and bad policy is as much to blame as the virus.
And now the CDC is trying to write off that trauma as an “algorithm error” when really they changed the algorithm to hide the trauma they created.)
There is no question that pediatric COVID is a concerning issue and kids are experiencing significant effects from Long COVID as outlined by Yale…
But the simple fact is they are unlikely to seek treatment or even know.

If you are a parent, then the Yale article sourced above has a lot of great info.
The critical idea for our purpose is that the risk is very high and the danger to our children will not be fully understood until they are grown. By then it will be too late.
For this reason, we are going to err on the side of caution but I’m going to explain that even when I don’t it doesn’t really alter the risk in a significant way.
For adults, the risk holds pretty steadily, a 25-day infection creates about a 30% risk.
We pull this data from a variety of sources but one particular study makes it clear.
Now, this has not passed peer review, which I’m aware of, but it’s a large cohort, 10,000 over 6 months, all had one shot of the RNA vaccine.
The reason we can use this anyway is because of the “Precautionary Principle.”
“The Precautionary Principle posits that, in the absence of certainty, the appropriate course of action is to err on the side of caution.”
So, if data comes in showing there is a GREATER RISK then it should be used automatically and the weight of peer review is to disprove the risk.
If the risk is REMOVED then the weight of peer review is to determine if the safety mechanism can also be removed and not until then.
If that seems foreign to you, that’s because we have been doing the opposite so far.
“This has been adopted by the American Public Health Association and the American Nurses Association… and the Principle has been incorporated into statements that describe the practice of public health nursing.”
If you are still concerned, here is a meta-data study showing how often studies are changed or retracted. It is very rare.
There is even a study from Feb 2021 where they explain that 30% of the infections had Long COVID symptoms 6 months later, this was the maximum follow-up time.
And like I said, we can pull this 30% number from a bunch of different places. I’ll even show you why getting caught up on that number is missing the point in a big way.
In regards to kids, a new metadata study was conducted to test for Long COVID risk across all available studies. Its findings found that the risk for children and adolescents was identical. The risk is stated at 25.24% for kids.
BUT those studies did not account for folks who don’t know that they have it because their life doesn’t have high cognitive demands or they are still developing.
More on this later… but we’re going to stick with 30% for that reason.
Here is the chart… It’s an excellent visual tool for understanding the risk.

First off, elephant in the room… Yes, that shows the risk of Long COVID having only had one shot as an almost identical risk to the unvaccinated.
I’m sure we can discuss a million variables about how the risk is reduced more with a second shot and a booster but it really only centralizes symptoms in your upper respiratory tract which is something we already see in breakthrough cases.
This offers limited, if any, protections for your brain and why so many people are arguing that COVID does not invade our grey matter. That denial is mostly guilt.
Now without getting too deep in and away from the subject, this happens because the current COVID vaccines available in America do not create a robust response in our upper respiratory tract… I cover this more in my earlier article… If you would like to read more about it you can do it there or I’ll cover it in another piece.
If you are reading this and are deciding to get a booster based on what I’m saying…
Yes, absolutely… Boosted infections have inevitably better outcomes.
Look at the hospitalization chart below as a relative generalization, not absolute.
But it gives a clear idea of how the current vaccines help, even if they have limits when it comes to protecting from Long COVID. You can in all likelihood afford one or two infections but save them for emergencies or accidents…
The damage is still significant.
And remember, if you are vaccinated… You might not even notice the first one.
But it might also be the worst sickness you’ve ever experienced.
So, it’s not very reliable for preventing infection or Long COVID.
Keep in mind, that this chart is for hospitalization not the severity of at-home illness. This means it helps prevent medical intervention, but you will likely still have an absolutely terrible time and that could come with lasting long-term side effects.
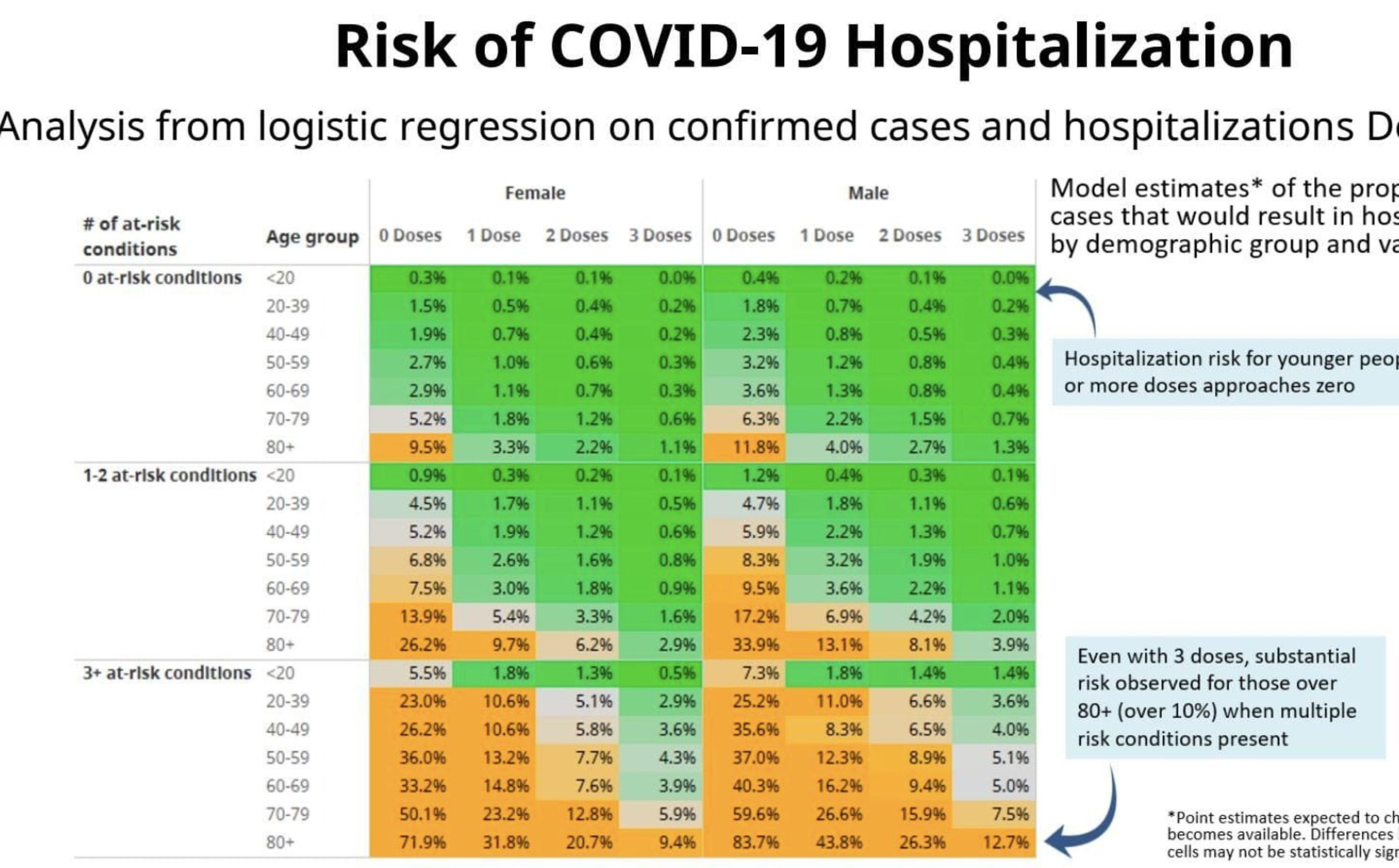
But the chart is clear. No question, get your booster. Outcomes are far better.
Also, someone asked in the comments if it was safe to get a booster AFTER having an infection and yes, this study says improvement is moderate but it is relatively safe.
More importantly, if you know anyone who is pregnant please beg them to get it. If there is one thing it does exceedingly well is that it protects the unborn.
Though it should be noted that as I was writing this more data came out from the CDC showing waning efficacy in the current round of vaccines. So, it’s important to be aware of their limits as we move forward into the next phase.
I know this is all very controversial to some people, so let’s not get bogged down in it.
And none of this is a reason to feel safe enough to risk infection.
Hopefully, when it comes to upper immunity issues this quote will suffice for now…

Vaccines are a critical part of our larger protection plan against COVID even if they came with some limitations… but they are the last step, not the first step.
And certainly not the ONLY step.
It’s even demonstrated in the infamous ‘Swiss cheese’ graphic.

On a side note, I hope for a speedy FDA approval for the Novavax vaccine that creates one-half of the antibody response we need to protect our upper resp tract.
There is a lot to be hopeful for coming up, which I’ll explain in an update.
Back to the chart…
So, the thing you might not notice right away is that the highest risk of becoming a long hauler actually happens in the first few weeks when your risk rises most sharply.
What’s happening is that the virus is in your body doing its replication process and that includes creating viral syncytia… (This is the biological process. There is a whole other layer to this about how it tricks interferons into not warning our B cells.)

Again, these are basically made out of clusters of YOUR cells. COVID does not create the cell matter, it invades, removes, and ultimately destroys your cells causing tiny micro-tears that we call inflammation as it rips them out of their natural position.
How tiny are these bleeds? So tiny that they can only be detected in the brain with a special MRI scanner called a “seven-tesla MRI.”

The virus is causing this damage anywhere it can get a foothold.
It’s kinda like in ‘Akira’… and if you have never seen that movie… you should… not even because of this… just because it’s beautiful and… you know what? I’m off subject… In that movie, spoilers, the final “villain” makes a body out of literally everything around him. This is what COVID does with YOUR cells. It hides inside, impossible to reach.
Because of this and other issues, our immune system is very slow to respond… and when it does the cells are hard to find. There’s even concern COVID could mutate so that it doesn’t leave S protein markers on the cell that makes the infected cells identifiable.
It really is as bad as it sounds.
COVID can hijack our cells and use our own hormones to melt into neighboring cells. The process is quite violent and rips your cell away from adjacent cells to be destroyed.
It can even likely hijack our mitochondria and use them in the same way.

There is actually data coming out that connects this to energy loss and shares problems that come with “Lyme Disease, chronic fatigue syndrome, and other post-viral syndromes.”

This is not the wildest idea because ACE2 regulates mitochondrial function in pancreatic B cells and we know that COVID can cause Diabetes.
The Doctor from the article was quoted as saying… "Normally, a patient should be able to extract 75% of the oxygen from their blood, but the Long COVID patients are able to extract only 50%.” That effect alone will radically disrupt your life.
And there is no known treatment for mitochondrial dysfunction.
In other words, there is no current method of recovery from this damage.
But how is this happening?
The reason that everyone thinks Long COVID is caused by some overly specific cell reaction that doesn’t match up to others’ work is that we are fundamentally misunderstanding the virus and how it attacks our cells then uses those cells to attack our other cells and continue the process, creating cellular ultrastructures.
And that alone is an autoimmune attack, so it can make any cell it gets into do this.
First, it finds an ACE2 or an Endolysosomes with Omicron and it invades the cell…
(I’m just going to refer to them as ACE2 because it doesn’t make a huge difference unless you are actually tracking the path of the virus and how it hijacks cells… Okay, so, if some cells only have Endolysosomes and not ACE2 then it could change the path of the damage but for our understanding, it really doesn’t make a difference.)
Then it can hijack the cell’s internal mechanisms and use that specific cell’s “tool bag” of hormones to access cells they normally interact with…
So, COVID hijacks the first cell, then that cell hijacks a specific cell that it has access to, and so on. Eventually, it gets into the lungs or brains and causes major and very specific damage that looks like another autoimmune attack…
But only after melting into a cell that has the ability to create that specific damage.
You can kinda see what I think is happening in the photo I pulled from this video. Though it’s not confirmed by the lab, one of the folks who is working on this team and is in the video said they were looking into the potential.
The dark clusters on the cell are visible, the cell literally looks infected, and has no elasticity when forced through the testing apparatus.

A healthy cell under the same testing has elasticity and should look like this.

When running this experiment, they are forcing it through a tighter area. The healthy cells flex and will change their shape but not the clumped cells.
The good news is the team from the video has a treatment that shows promising results but the bad news is these treatments are still far from being mass-produced. But their treatment removed symptoms entirely, returning folks to “normal.”
This is in all likelihood one type of the Micro-Clots we hear about. Those are not only loaded with viral matter, but they also clog up your circulatory system causing a very deadly illness called “silent hypoxia” because it happens without breathing difficulty.
These “clots” literally jam up your narrowest capillaries…
Plus, wherever they burst is where you get COVID damage.
And that could become Long COVID symptoms.
(Update: There is another type of Microclot as well called ‘Amyloid Fibrin Microclots’ that can form in the brain and the bloodstream post-infection, but I left it out because it’s a type of Long COVID symptom not a risk factor for Long COVID itself…
This type of Micro-clot jams up your capillaries Post-Infection clearance.
I have theories for those that I will discuss in an update but for our purposes now, we are going to focus on the MicroClots that are a risk factor for Long COVID.)
Even in this study, they are being referred to as “inflammatory micro-clots.” That should sound familiar at this point.
Shortly after writing this article another study broke explaining a similar story, that autoantibodies are triggering the clotting behavior. Their findings were not conclusive but it sounds a lot like the cells’ abilities are being weaponized by COVID.

We will chase our tails forever if we don’t understand this because it’s not ONE of these things happening… It’s ALL of these things happening.
COVID basically gets in the cell and turns everything up to 11 until the cell dies.
This causes every variety of auto-immune attacks in different orders that can appear extremely chaotic. Which makes our testing results equally chaotic, but it’s in a chain.
Omicron does it slightly differently but the outcome is the same, the method of getting there is just different which is what makes it seem mild, but it’s really not.
Now, we have other auto-immune attacks in addition to that but it’s too much to get into right now. We’d have to discuss every mechanism in the body.
But it’s really important to visualize what is happening here…
That’s from an animal that is more effective at fighting off this particular virus.

The video only gained notoriety through a contest that Nikon was running.
If you don’t think important science isn’t being held back, look no further than groundbreaking science only being seen because of a photography contest.
Ms. Aicher specializes in zoonotic diseases and hoped this would “demystify the virus.” We need to understand what we are really up against.
Or else, we simply can not understand the risk.

Now, remember, Bats don’t get sick from Coronaviruses, at least they don’t show symptoms… but clearly, it has no problem destroying their grey matter.
When COVID infects you this process happens inside of you.
The damage it creates is known as Long COVID.
Persistent mutating virus exacerbates this situation.
If it gets completely out of control, you die.
Probably the best way to think about it is death by a billion cellular cuts…
And the worst way to think of it is that the virus is eating and digesting you.
Technically, it’s slightly different but both are true.
Think of your lips getting chapped, then so badly they bleed… but in this case, the matter is being turned into something that creates more of itself and it’s doing it INSIDE YOUR BODY. It’s even a similar mechanism to what herpes does.
To break the idea down even more simply, the important factor here AND WHY COVID IS NOT LIKE THE FLU… Is that COVID does not have to leave a cell to enter the next one… This means your immune system either has to wait to fight it until it bursts or they have to train our T cells to fight our own cells to get access to COVID and we don’t want that to happen… I’ll explain later in the article.
There is even a great zombie reference here because the cells it hijacks are essentially zombie cells and have all the powers that come with being that cell but our body has lost control of them to the virus.
So, imagine a superhero becoming a zombie and keeping their superpower…
Our cells each have different ‘superpowers.’ COVID can hijack and use that power to damage our own cells. ‘Nuff said.
Our cells and extracellular network all have different abilities or types of organic chemicals to release. Now imagine if they released both the good and the bad ones at the same time. This leads to a massive Cytokine release from our own hijacked cells
This is one of two confirmed autoimmune attacks happening in the body, even though this is technically EVERY possible kind of autoimmune attack that your body can produce because it can hijack ANY cell … Though here, it’s just one type.
But, technically, everyone who was betting on Zombies for this Pandemic kinda won, they are just really really tiny… and inside you, which I don’t think anyone saw coming.
When the viral syncytia bursts it’s like a tiny zombie starter kit dispersing in your body. But more importantly… Which is kinda hard to believe after that take…
All of these create a variety of EXTREMELY complex long-term issues.
Now is about the time I mention that when we talk about the risk from Long COVID we are actually discussing how close you are to death…
It’s the same chart.
The big point that is going unsaid in this is that this advances existing diseases. So, if you have heart disease and get COVID it will make your heart fail faster.
It can do it by simply occupying your immune system or adding to the damage.
This is why the narrative behind death “With COVID” or “Of COVID” is fundamentally misunderstanding the risk of COVID.
COVID is what is known as a “Threat-Multiplier” in the same way Climate Change is.
But in your body, this means something very specific…
COVID ADVANCES EXISTING ILLNESSES THAT MIGHT BE UNDIAGNOSED.
This can give you a bit of a window into what to expect from Long COVID damage in addition to all the other normally expected symptoms.
This data shows the increased risk of all types of disease post-COVID infection…

This is just one of the charts you will find in that study, there are four more.
And to be clear, that data is for DELTA BREAKTHROUGH INFECTIONS.
Omicron infections have been MUCH more common.
Simply put, everyone is at risk… and if you have heart disease already…
Here is a heart-specific chart to help you visualize it, this data is a year post-infection.

COVID and heart disease make your heart disease that much worse.
If someone dies of a heart attack and tests positive for COVID then COVID prematurely caused their death because we can live with heart disease…
But we cannot live with COVID.

I bet it was that study where they got the idea for “herd immunity” as our necessary path forward but all they ended up doing was “thinning the herd” instead.
The difference? ‘Herd immunity’ is immunity through vaccination while ‘thinning the herd’ is immunity through infection… Which one do you think we are doing now?
Before I go on…
There are a few misconceptions about COVID.
#1. You do not gain long immunity to COVID from an infection.
A significant amount of studying has been done to compare cross-immunity.


The theorized variants have already emerged since that study was published.
More on that in a bit
But the logic behind the 90-day rule on reinfections is actually pretty upsetting.
Here is the UK’s reinfection chart… The only reason they can get away with saying Omicron protects you from Omicron is that they have set a rule that reinfection can only occur after 90 days… Many Countries and States have this policy.

This means THEY KNOW the virus will LIKELY persist for as long as THREE MONTHS. But in reality, if you reset your acute infection phase then you are likely reinfected. This is another reason for minimizers to push against genome testing.
This chart is going to skyrocket soon because the 90 day limit on reinfections is up…
And this is why the UK is stopping testing.
#2. COVID primes your body for future infections.
It damages our B cells, T cells, and our general ability to fight disease.
And that B Cell link talks about it causing Type 2 diabetes as well.
The hormone-induced cell death is also happening with T cells.
#3. An actual COVID infection happens in a few stages… It’s a lot different than how we visualize it and certainly not within the recommended five days of isolation.

(Update: When I say that very few people understand this even though it is critical for understanding the risk associated with a COVID infection…
Here is the two-time and current Surgeon General explaining on Twitter, MARCH 1ST, 2022… That his family’s infection is over after two weeks.

I can not make more clear how undervalued this simple fact is in our current policy…
Which is also strange because this fact leads our reinfection policy to prevent driving our numbers up to fast when folks get reinfected after a month but is ignored when it comes to recovery or the risk of Long COVID from multiple infections.
This policy is being used only to help hide reinfections but ignored for recovery.
It takes a full three months to clear the virus… T3 is 2-3 months post-infection.

This is why some symptoms appear later because the virus is still damaging your cells and it can do significant damage in that time, settling in all kinds of strange places.
It is possible he received advanced anti-virals but most will not have them available.)
This really really really matters because if you noticed in the chart for risk of long COVID earlier that risk is determined by…
DAYS OF INFECTION AND NOT THE SEVERITY OF SYMPTOMS.
So, being vaccinated is great for keeping your symptoms from advancing but you are still infected for that time, and though at first, that seems like it should significantly reduce your risk… I’m sorry, no. The change is negligible. I’ll show you.
Though it should be said, how ever your days of infection are reduced, the lower your risk for Long COVID will be. That may seem obvious, but I had to explain it this far in.
Getting double vaccinated could possibly shorten your first infection and that means fewer days infected and less risk of Long COVID… but that protection is short-lived though it does give you an advantage here in every way over the unvaccinated.
It’s important to note that in that brand new UK study I just added as a source, even though the risk was reduced for SOME people for others it was not.
Headlines like these that speak relatively do not tell the whole story.
Less than, greater than… It’s like a study that doesn’t show (n=) at the start is probably trying to trick you.
Folks are not great at relative conceptualization and they take advantage of it.
That’s right around when the confirmation bias kicks in.
Sounds good, right? Well, you might want to slow down for a moment.
Even with those very exciting headlines, double-vaccinated folks are still getting Long COVID and suffering needlessly. We also know these vaccines wane, so it’s not a great time to get rid of your masks. If you haven’t upgraded yet to Kn-95 or better, please do.
Also, it should be noted that in the UK they are referring to what we are talking about as Long COVID as “Post-COVID symptoms” and Long covid in the UK means extended acute symptoms… So, they are only talking about the initial infection.
It’s a bit misleading… and that can be deadly.
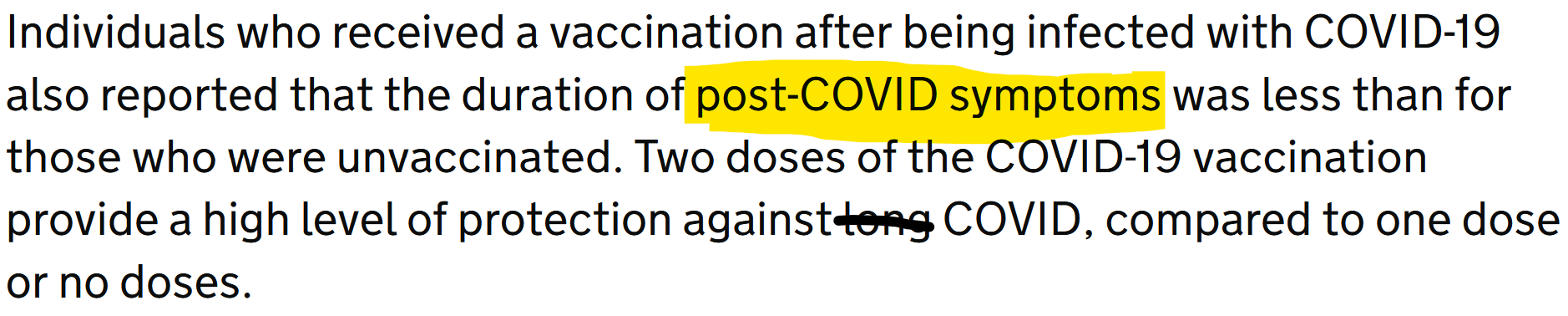
This is why we need standardization with these definitions but the actual results they are presenting are directly in line with what I’m saying here which is why I used it.
This headline is a reason to get vaccinated, but it only temporarily reduces your risk.
A more realistic representation of risk comes from this recently released study explaining the efficacy of the fourth shot against Omicron.
And it’s not great.
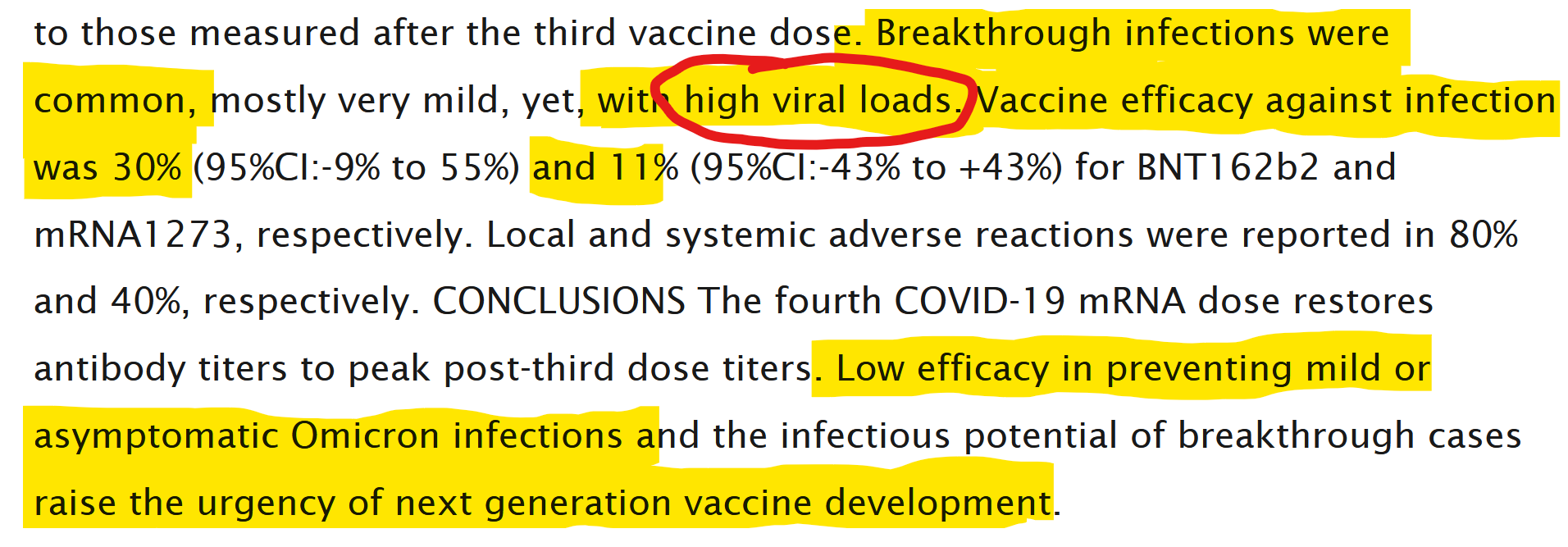
The 4th shot returns antibody support to 3rd shot levels but breakthrough infections were common and still allow for HIGH VIRAL LOADS… Mild or not…
They had hoped that something like this would happen and the IgG response would get high enough to prevent infection. It requires a very high response to do that.

Sadly, that did not materialize. It likely means it needs to be applied locally.
That means intranasal vaccines will be needed.
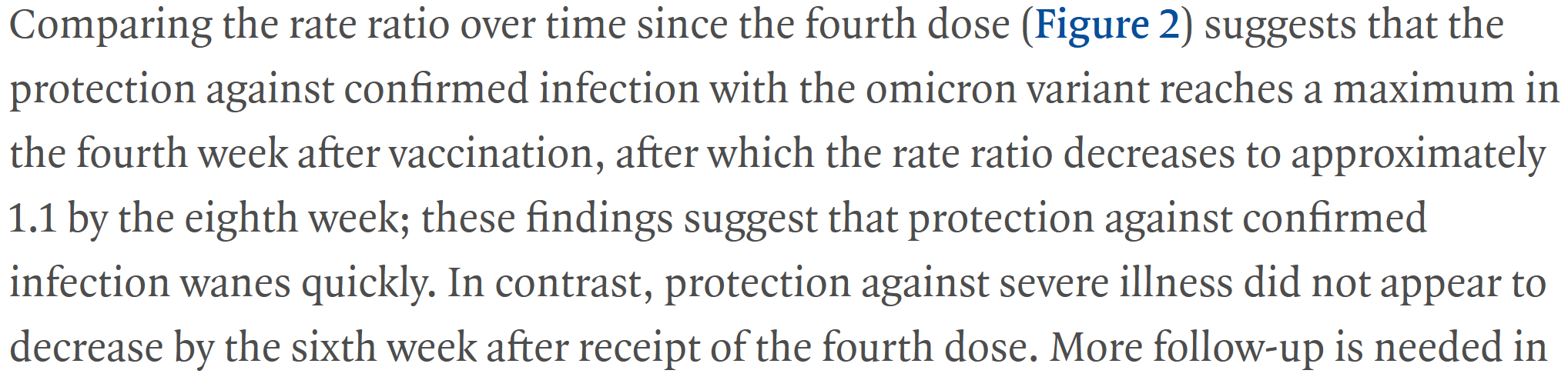
Even more data has come in showing the support from the 2nd Booster or 4th RNA shot, keep in mind… it’s all the same shot in different volumes… drops off very quickly.

So good news first, it does appear that the RNA boosting does maintain its protection against death… Though this testing period was very short, just less than 6 weeks for testing severe illness when we know Omicron has delayed severity. So, the reliability of that may be limited, though better than nothing if infections are unavoidable.
But the actual bad news? Protections waned faster than the third shot.
This is probably why the WHO lead said that we can’t “boost our way” out of this.

And to be clear, it can and will mutate in vaccinated populations until it is fully sterilizing and then we can work toward actual herd immunity.
This gif from Twitter perfectly encapsulates how it’s supposed to work.
What we are doing is nothing like this.

But most importantly this all means it still won’t prevent infection…
And that’s all that matters when it comes to the applicable risk of Long COVID.
It should be said that even a “mild” case can lead to “multi-lineage cellular dysregulation and myelin loss in the brain.” This is a type of Brain Damage.
And that’s without COVID even entering the brain.
This likely happens because of our organic cytokine release from infection and I will be expanding on it in a later update.
If you are concerned and only have the RNA available to you still… Here is a chart.
The Moderna and Pfizer vaccines use slightly different processes so for the strongest results, mixing them is the most effective.

Though when it comes to your risk… It must be said…
There is no circumstance where being vaccinated alone will prevent you from catching Omicron. You must continue not sharing air until Novavax and an Intranasal Vaccine are approved, we need a combination of both, or you will continue getting infections, continue building your risk of Long COVID, and ultimately lead to Death.
Even Novavax will not be foolproof and will require a combination of prophylactics and it’s still not clear which intranasal will be our winner or if Novavax will hold.
But don’t get confused… Even with RNA vaccines, you will do better if infected.
There’s no question if you are vaccinated and you do get infected, you’re more likely to have a better outcome than an unvaccinated person but the risk of LC is still present.
So, here is the bad news.
We think of infection like, we get infected, and we recover then we’re good as new, protected for some amount of time.
But not with COVID… even in a mild case.
With COVID… First, it takes months to fully recover, and not only do symptoms of Long COVID develop months after the fact, it mutates so fast that the next variant you encounter might have the same name but a completely different immune escape.
That means exactly what it sounds like.
It’s already known that in one infection, Influenza, as an RNA virus, can mutate enough to be unknown to the body’s immune system… and that citation is from 1982.

I can get really deep into this in another update and I touch on it near the end but here is a great study on its mutation rate. We have since found it to be even faster too…
Just as a quick demonstration… Here is an example of a doctor who acquired COVID from a donor's lung while preparing it for transplant… Keep in mind, that the donor passed every COVID test the entire time.
And even in just that one single transfer, it was a slightly different virus.
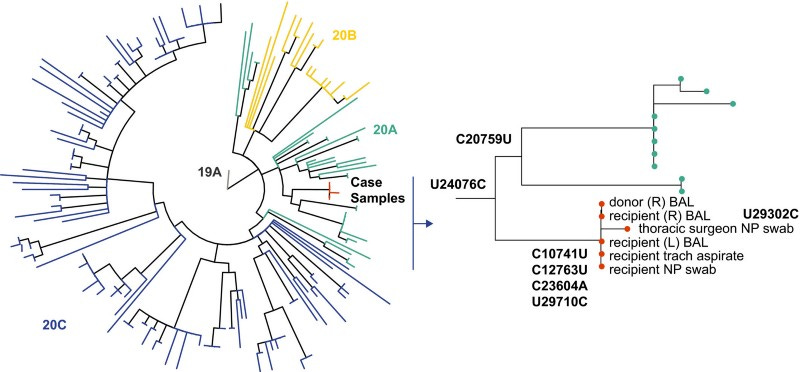
I hope we can move forward with this as an understood idea…
COVID mutates between each person… Sometimes a lot, sometimes barely at all.
But within a few weeks, the variant introduced to you will be different.
Let’s run some more of the variables.
Now, since the infection process is at least a month, I was actually being generous by saying 25 days earlier which means you can’t technically get reinfected in that time…
The Australians tell their people anything after 28 days can be considered reinfection.
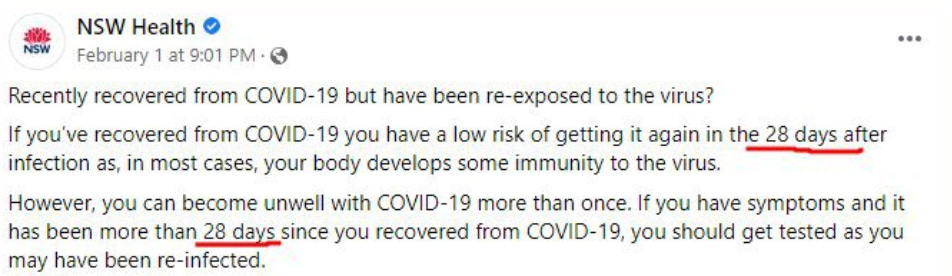
First off, that bit about immunity… Not quite…
Second, you can still get infected with a second variant… At the same time.
In HIV this is called a “Superinfection” and this term is easily applicable to COVID.
This can do all kinds of bad things.
Isolating while infected is as much about protecting others as it is making sure you don’t get infected with a second variant.
(There is one other important reason too, I’ll explain at the end)
Basically, through Genetic Recombination, they can combine and create new variants if the two variants infect and occupy the same cell…
And with 10 COVID cells per human cell during infections, odds are pretty good on it.

It used to be rare, but as things have sped up… now it’s less rare. This writer refers to it as a ‘recombination event’ as he discusses that he thinks BA.3 was birthed from BA.1 and BA.2 recombination. BA.3 is now being called XE.
XE is now considered one of the most infectious viruses to ever exist.

And while it recently got renamed… BA.3 has been around in Germany for months.
I’m sure there are differences, but there is a lot of effort to confuse the public over this.
We saw the same manufactured confusion frequently with AY and P1 variants.

COVID has been doing this the entire time but it’s hard to track unless it happens in very specific ways but we are getting better at it.
This particular Twitter account tracks them especially well.


It’s important to realize that all RNA viruses can do this.
As a matter of fact, there are a few things ALL RNA viruses do that we seem to have forgotten which increase our risk… Like multiplicity reactivation, for example.
COVID’S reactivation process is likely similar to “Multiplicity Reactivation” in flu.
This is likely the process by which the virus can reactivate that I mentioned earlier.
Here’s an example of how the flu does it… Keep in mind that COVID is not the flu when it comes to risk but a lot of the mechanics of RNA viruses are similar.
The Furin Cleavage site in COVID is what makes it so different though.

Two “beaten” pieces of RNA can recombine if enough of the virus is alive on either RNA strand and they occupy the same cells.
If two of the same RNA strips infect the same cell and they can recombine to make a new COVID cell, that could likely mean a new variant that you have limited, if any, immunity to… We have case data on this now.
But, that’s not all folks… Next up is Horizontal Gene Transfer.
This is when RNA or DNA from one species slides into the RNA or DNA of another species…AND ALTERS OR POSSIBLY EVEN CREATES A NEW SPECIES.
This is the ultimate “slide into someone’s DMs” except it’s their DNA instead.
That could mean COVID’s genes could jump phylum or it could pick up genes from other organisms… and I’m not joking.
We wouldn't even know what it would look like.

And it was only in 2010 that it was discovered that MANY microbes perform this activity a HUNDRED MILLION MORE TIMES than previously thought.
So, our understanding of risk here is kind of… bad.
The simple fact is that Horizontal gene transfer in microbes is much more frequent than previously thought and it’s so new that it hasn’t been adopted broadly yet.
It might actually boost or be boosted by another virus or creature in ways that we do not yet understand… and we barely understand any of this, far from making applications.

Life is not a Michael Crichton book (RIP).
Science is barely figured out and even less is agreed upon.
But this data had two very important pieces of information.

Microbes can do it overnight and antibiotics can trigger it in bacteria.
Guess what we are using on COVID in desperate situations..?
Probably very similar Antibiotics… If people are eating horse paste… Don’t do that btw… Then it’s very possible that ALL TYPES of antibiotics are being used.
And then we get a new species… It might have already happened.
And, yes, COVID is a virus, not a bacteria but this is so poorly understood and we know viruses do it too even if it is slightly different.
Truth is that viruses have always been changing our DNA and have been critical to our evolution but none, that we know of, have been as dangerous as COVID.

Literally, half of your body is made up of viruses.
380 Trillion of them.

It’s actually more than half your body.
That means, more than half of your body is not even you.
We have almost no idea the role the viruses that we coexist with are having with COVID… Is COVID wiping them out and that causes its own form of Long-Hauler Syndrome that is even harder to fight off?
Might one aid us in our fight with COVID?
Is it possible that our damaged immune system might allow our own viruses, which have a better understanding of our body, to work together to create new superbugs?
We’ve already seen COVID “awaken” Epstein-Barr from our DNA and we know that Epstein-Barr is tied to fatigue-related symptoms we see in Long COVID.
To say this is poorly studied is an understatement…
As far as I can tell, it’s barely studied at all.
We know almost nothing about more than half of the living parts of your body… Because they aren’t actually your body.
But they are part of the system that keeps it functioning.
And your Immune System is what keeps it all in balance.
But really. bacteria, viruses, mitochondria, etc… Are PART of our immune systems.
And we know almost nothing about their interactions unless it kills us.
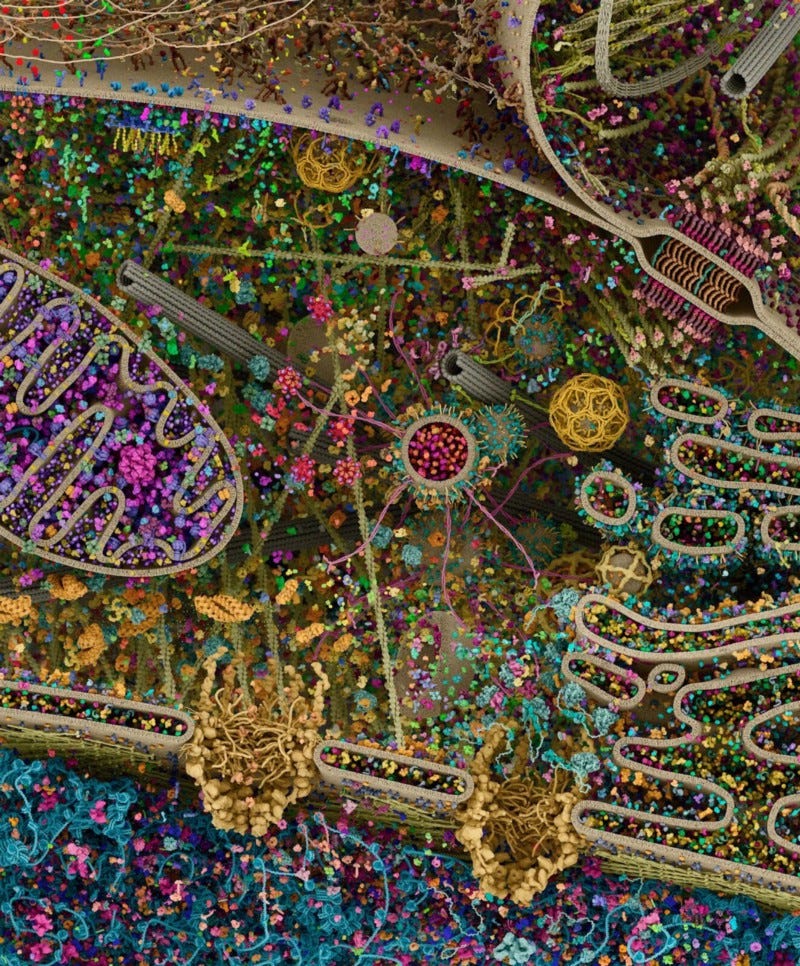
They have gone far enough to identify everything in these pictures and you can go to the site and it’s interactive, really cool stuff.
But how much of a risk does this really pose?
Well, there are more viruses than stars in the universe. So, the potential is there.

If this sounds far-fetched, that’s not unreasonable.
Most of this is relatively new and has only not been science fiction for about 30 years.
Shortly after writing this section… COVID started displaying itself as Hand, Foot, and Mouth disease in children living in the Toronto area. It’s localized, so far.
This could already be Horitonzal Gene Transfer occurring. Keep in mind, that the CDC wants kids to stay at home when they carry this disease.
Makes you wonder why COVID is allowed in schools.

This could get even more out of control and very quickly.
Basic logic would propose that if we have this many viruses in us operating at any given moment then it speaks to the reality that not only COVID but all pathogens could be using these access points… assuming they have access.
And we know COVID has access.
The longer we allow COVID free reign in our cellular structures, the more of these Horizontal Gene Transfers (HGT) events that will occur. There is no limit to the potential for the havoc it can cause to our bodies and immune systems.
Well, until you die… That’s the limit.
But until then COVID has the potential to evolve wildly if left unchecked.

These events will likely lead to higher transmission rates and higher viral loads which increased the length of your infection and consequently your risk of Long COVID.
Also, it is almost assured that the next variant will have immune escape to it.
We often see antibody tiers as reactive to different variants in testing, but because of immune escape, that data can have limited real-world applications.
And this can misrepresent the risk.

As testing decreases, we actually need to be ramping that up to include genome testing… We are going to be flying blind without this data.
While the simple fact is that we are already seeing the outcome of these events.
It’s theorized that Omicron was birthed from HGT from the common cold because it picked up genes specific to it which increased its transmissibility but also brought new variables relating to the common cold specifically that we saw in the media.

It’s hard to talk about how different Omicron is and not seem hyperbolic.
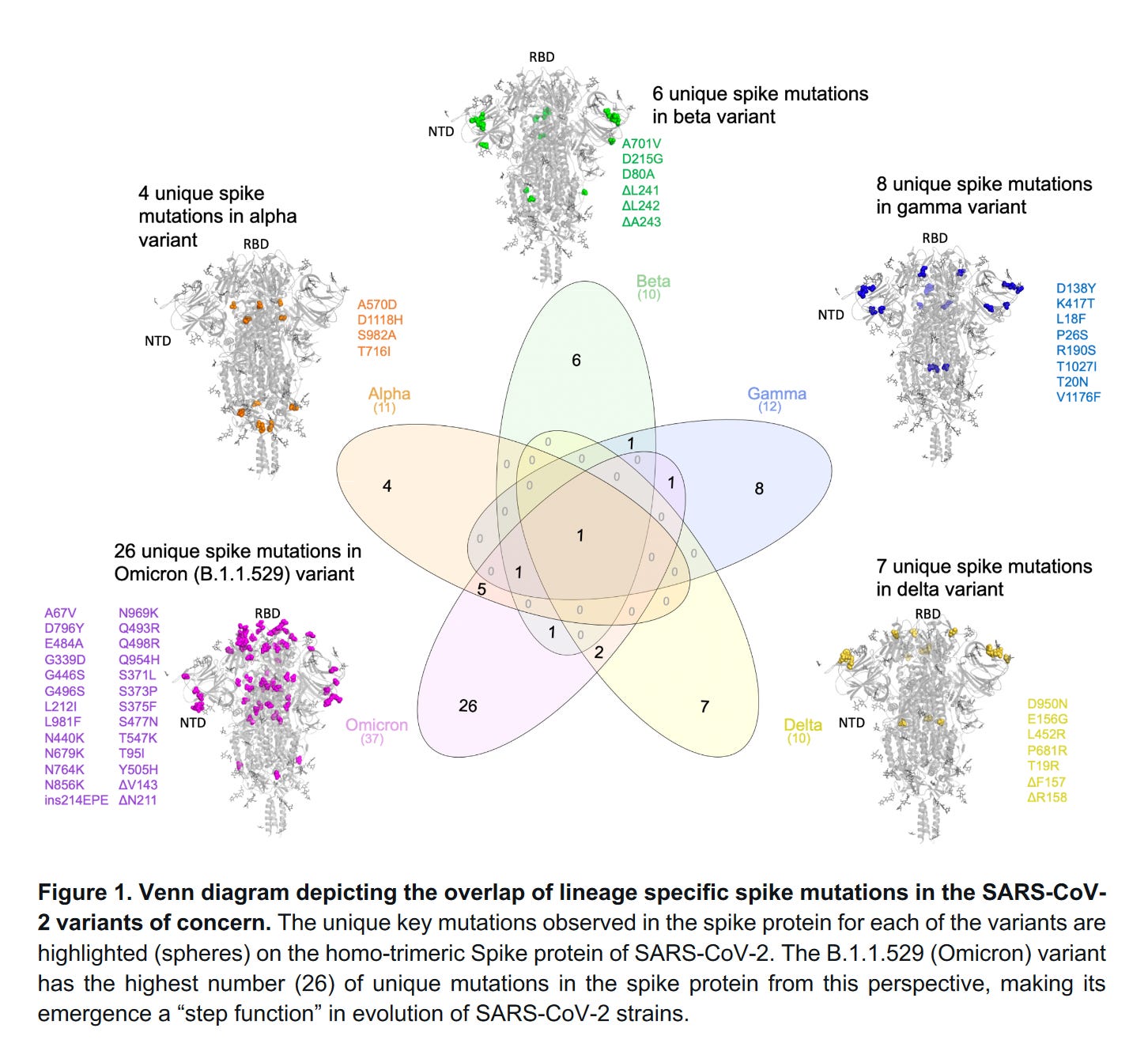
Here is a “map” of Omicron’s mutations compared to previous variants.
It has 26 unique mutations which is a significant jump in unique mutations.
But this gives you a good idea of why a previous infection offers little protection.
It’s undeniable that recombinant event becomes increasingly more common as we remove mitigations, stop quarantining, and the incubation rate shortens.
This is the transfer point from BA.1 as it becomes BA1.1. post recombinant event.
B.35, an Alpha variety, combined with BA.1 to make BA1.1529.
If I can find it again, the South African data shows a narrow line of Alpha in their RNA sequencing charts from the time… There had been an older Alpha variant bouncing around Africa unmutated for the entire Pandemic.
That’s to quell any conspiracy theories, the data explains it perfectly.

Here is more data from the previous study showing the significant jump in mutations and how that relates to differences between Delta and BA.1.1.529.
That big blue line is the average number of mutations in sequenced genomes.
That’s a significant opportunity to create immune escape.
This is how Omicron reinfects so easily.

And it gets worse… Though BA.2 is considered an Omicron variant… Not really.

To give you one more visual conceptualization of how far out we are…
All of the red is BA.2… Well, we think it is. It’s supposed to be.
It all changes very quickly.

This chart is the entire pandemic charted by unique mutation.
It’s actually a really impressive website.
Each one of those is counting unique mutations and with this last Horiztonatal Gene Transfer we went way off the charts.
This chart is really only designed for 70 mutations but has room for 90.
And it’s over that.
We’re going to have to change the metric for counting mutations at this rate.
We can only assume this will happen again and it doesn’t even stop there…
Then BA.1.1 combined with BA.2 and that made BA.3… now called XE…
Which brings us full circle… Hopefully, that demystifies Omicron a little bit.

This has led to a number of mutations beyond even these.
Consequently, we’re seeing a wide variety of symptoms and it can get very confusing.
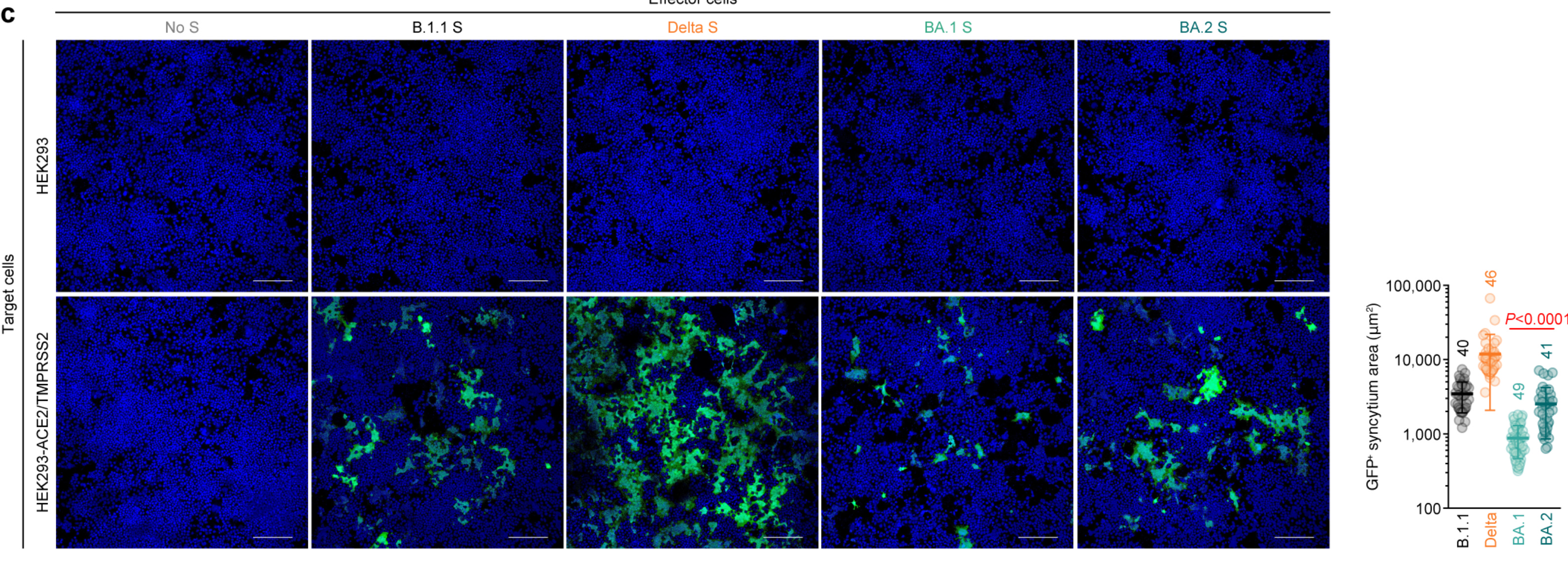
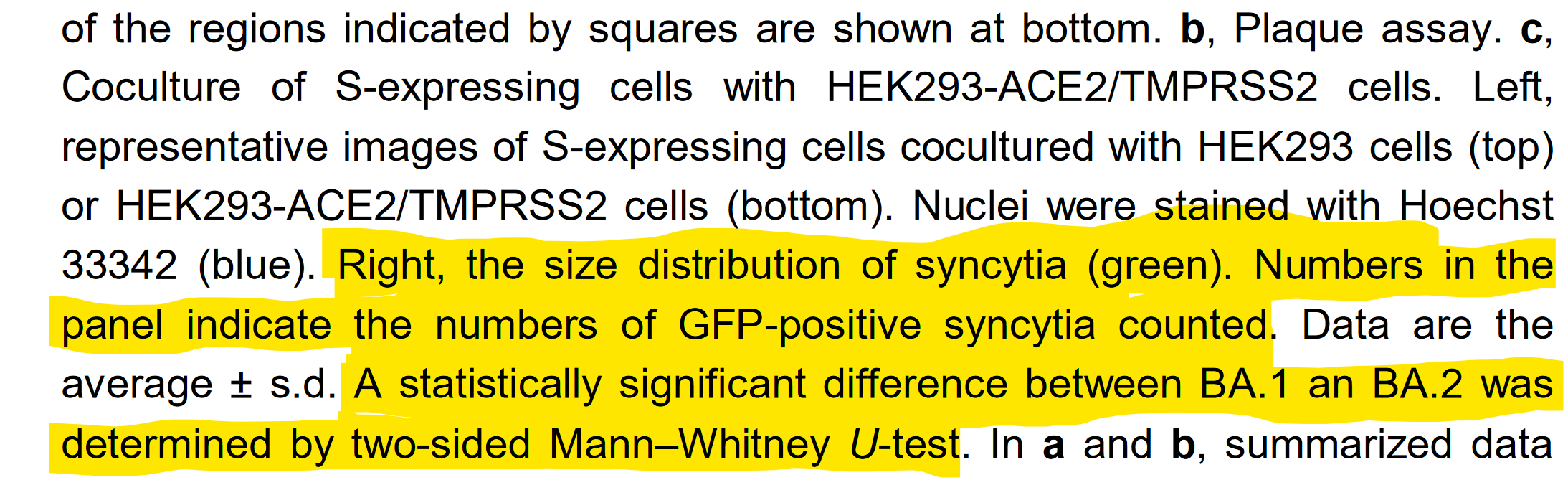
For example, while BA.1 had trouble holding syncytia, BA.2 does not…
And when we say that BA.1 had “trouble”… It does NOT mean it couldn’t do it at all.
Here is a comparative chart to give you an idea and keep in mind… Deltacron is real and we are heading back toward the direction of that level of syncytia forming.
This process kills your cells and causes the damage known as Long COVID.
So, BA.2 is ready to destroy our lungs again, but we aren’t collecting any data.
And now we are getting anecdotal reports that symptoms are more digestive.
So, we’re getting that flashback to the early waves where toilet paper was essentially currency but very little of this is being openly discussed with the public in clear terms.
(I will be expanding on Deltacron and the risk of the Merck drug potentially making these events more common in a future update... TL;DR: Don’t use it.)
And this all matters for assessing risk.
See, we think of “science” as running at 100% but it's really at around 60%…
We are barely even capable of distinguishing between an infection, reinfection, a superinfection, or a reactivation… Sadly, applications from these studies are rare.
This data is actually really important for understanding why we have come to expect a 14-day resurgence post-acute infection because, on average, the viral syncytia can hold for as long as 14 days post-infection…
This means that not only do you have a secondary acute infection between 10-14 days post-acute infection, but COVID has plenty of time to mutate for immune escape.
COVID doesn’t do this intelligently, we think… Well, we hope.
It simply produces so many mutations that one will be different enough to avoid your antibodies and evolve to become the new dominant based on immune escape.
This is why relying on your immune system alone to beat COVID is not a great idea.
Remember COVID is producing millions of itself to hold that 1-100 Billion Viron number we discussed earlier… and it only needs ONE to develop immune escape.

This particular quote has three things going on in it…
First, it validates my 14-day timeline
Second, it discusses ‘paracrine senescence.’ You might have noticed I mentioned “hormone-induced cell death” without an explanation a while back…

This is the method that COVID uses to target other cells using the hormones of our cells to get them to open our other cell’s ‘doors.’
Paracrine is the targeting of another cell…
Senescence means cell death or losing power.
So, we know this means the viral syncytia is likely intact and still killing cells.
The third is “The sustained infection-induced paracrine senescence described here may be involved in the long term inflammation caused by… infection.”
That’s viral syncytia being described by its mechanics.
It’s possible, even likely, that Horizontal Gene Transfer is occurring in these exchanges. This creates the perfect environment for that interaction or event.
When I combine this data with our anecdotal evidence and the timeline for infection means viral syncytia could traditionally likely hold for about three weeks assuming it was intact before you began gaining the short-lived immunity to that exact variant.
And that’s a lot of time for things to go wrong.
BA.1 was not as good at this but that could lead to worse outcomes in the long run because it overextends your immune system by putting the virus in so many more places which is more places to have damage which means more places to have symptoms. It would also turn Omicron into a slower burn, which we are seeing.
And even after you develop a T cell reaction to the virus, you still have to wait for the viral syncytia to burst and allow your Immune System to fight it or else we end up, possibly, training our T cells to fight our own cells… Which could lead to all kinds of complex inflammatory issues just like the ones we are seeing or, worse, using up or killing our naive T cells which we appear to have a limited supply of and are directly connected to aging.
That last part is very bad… It can not be overstated how bad that can be. My theory is that the viral syncytia can maintain longer than it takes us to train naive T cells into effector T cells. That could lead to our own cells being put on the memory T cell list.
So, for the next six months or so, possibly forever, your T cells could identify your own cellular structures as an invader… and try to fight it, causing more inflammation.
In Children, if this happens in the brain it can easily lead to death.
Sadly, that young lady passed away.
This is likely the second type of autoimmune attack that can also seem like persistent virus but is our own immune system being trained to see our cells as an invader.
And again, the virus can still mutate immune escape while it’s hiding out in your cells.
Plus, every time the viral syncytia bursts it’s like COVID dumping an RV full grey of and black water directly into your body… The S protein material alone causes issues.
And that includes that ‘zombie starter kit’ I mentioned earlier which is just basically newly developed virus ready to have that house party in your organs we talked about.
That means, if your immune system can’t mop up all the loose viral cells then they find another ACE2 and starts the process all over again… One more time, BA.2 is not having trouble holding syncytia as BA.1 did.
But this is more of the “persistent virus” that everyone keeps mentioning.
Though it should be said it still has a few more flavors of which all are problematic.
So, a damaged immune system means you are in a lot of trouble, and COVID damages your immune system.
That makes a COVID infection the comorbidity everyone is forgetting to track.
Because of course, comorbidities factor into this as COVID is likely to exacerbate whatever existing issue you have as well as make your risk higher overall.
For those that are interested… This study lists hypertension, obesity, and diabetes as the three comorbidities most commonly seen in COVID patients, in that order.
A study recently brought even greater clarity to the risk of diabetes in general.
It uses a very large sample size and they display the risk is 1 in 50 who get infected with COVID will get new-onset Diabetes.
Every day millions of people play the lottery with astronomical odds…
But they can’t process that their chances of getting Diabetes are 1 in 50.
In addition to that, it’s a 1 in 50 chance of getting the #3 top comorbidity that puts you at risk for greater COVID damage or death.
And this all matters for explaining risk…
Because we already answered the first question… It’s 30% for a 25-day infection.
And to be clear, the ‘25-day’ is an estimate of the average length of infection when you include incubation, acute, and post-acute… I’m being pretty reasonable with that number. Even though you might not be contagious, you are still infected.
That means the question everyone wants an answer to is…
What is the risk of multiple infections in a short amount of time?
This is the big question no one can answer or they don’t want to…
And I can see why.
Here is the really bad news.
If you don’t have a significant amount of time between infections then the risk COMPOUNDS on each infection…
The question really is… “What is the entropy rate to risk based on recovery between infections?” That means, how quickly is risk reduced over time?
Well, for starters you can’t even start the clock until the infection is done, and assuming you have a standard ‘mild but not actually mild’ case… It’s at least 30 days, but to be kind we will stick with our original 25… You will see, it won’t change much.
Because the real problem is that in some cases the virus is detectable in your blood for 2-3 months post-acute infection… Washington’s 90-day rule, I mentioned earlier, is enough to validate this.
That means your recovery entropy doesn’t even start until the virus is cleared and then actual recovery can be slow. This process can vary wildly from person to person.
(Update: We’re learning more about COVID every day, and part of that includes our biological reaction. A big part of that is the cytokines that both get released by our cells and the cells COVID hijacks… In even a “mild” case.
This alone leaves a 5-month “scar” on your system and macrophages.
Assume you need a minimum of 5 months to start your entropy-recovery process.
It’s documented that multiple infections inside of that window lead to worse outcomes and more ICU visits… Which will eventually lead to death instead.)
So, what happens if you get infected again inside of that window?
Well, your risk springs up again just like it did in the first infection… but starting from where your recovery entropy brought down your risk and it won’t be much.
This is the part when your risk increases the most in the shortest amount of time.
So, the risk is 30% per infection compounding if you don’t have sufficient recovery time between infections… Required recovery time could be 4 months or 4 years depending on the situation but either way, it’s slow.
Plus, if you have comorbidities, which we all do, then that risk is can be higher.
Even under the best circumstances, recovery entropy starts at 5 months.
That’s the best possible scenario to get the virus cleared and recover from cytokines.
Then actual physical recovery?
One study showed that 91% of folks that were tested need 35 weeks of recovery.
In another, it says that 6 months later 50% of COVID survivors had Long COVID.
Combined estimate?
It’s a minimum recovery period of 4-6 months for an asymptomatic infection.
1 year+ for a “mild” case that experiences basic symptoms.
Several years for an average at-home “bad case.” These folks are often long haulers.
Staying in the hospital for extended periods can cut your lifespan down dramatically, but not always dramatically… Though it will shorten your life.
As I finished my last edit a study broke that explains your risk of death increases a huge amount compared to the control post-COVID infection…
But my biggest takeaway is that the risk does not significantly reduce.
And that chart is for a whole year.

This study pretty much makes the argument that there is no recovery entropy post-infection inside of the first year… but for sake of argument, we are going to keep going.
And to be clear, that is far worse than what I am calculating.
How does this relate to our schools?
Let’s say, these kids in school or teachers are getting multiple infections…
Not only does each one get progressively worse but their risk of death gets higher…
Because it’s based on damage done by the virus in a fixed amount of time.
Now, when I mentioned the ‘coordinated symptoms’ this is bad because if you spread the virus all over your body the damage might be less than if the virus gets centralized in one organ… It’s the same amount of virus… It’s just all in one spot now.
You are literally trading ‘variety of symptoms’ for ‘severity of a few symptoms.’
Before it would centralize in our lungs and wipe those out, and still does to the unvaccinated regularly, but Omicron isn’t doing that.
So, the effect that might take multiple infections to cause significant damage, now it can do that damage to one organ… and that organ seems to be the brain because of the lack of protections in the upper respiratory tract and the change from Omicron.
If you haven’t noticed, both outcomes there, the one I listed earlier and the one right then, are both terrible.
Back to the risk
So, you get two infections back to back… and you had one infection slightly longer than the other with no recovery time between them then your body has not had time to heal those billion tiny little cuts that we just call inflammation, but, again, that’s what it actually is… Just little microscopic cuts, in this case. (Disclaimer: this is not the ONLY type of inflammation, but the story is similar… A lot of these cells also release cytokines and these cause inflammation as well.)
(Update: It looks like the reason Omicron looks milder at first is that it doesn’t hijack Interferon producing cells as well. So, this means there will be less initial disease.

But INITIAL is the keyword there, as we are seeing with Omicron taking longer to produce fatalities… This is likely happening because the interferon-based disease that is among the most easily understood biologically is less at the start. Until it works its way around to a cell that can hijack those cells and then it does the damage.
To be clear, interferons are a type of cytokine.
This gives us more time to fight the virus but because it also makes it seem less dangerous, we do less to treat it and the eventual outcome is the same.
So, while the changes to Omicron make its incubation rate faster, it also makes its eventual path to death take a few weeks longer and because of the circumstances, this means the risk of death is even higher as folks dismiss the risk.
This also means more days of infection and likely a higher risk of Long COVID.
This means Omicron infection does not lower your risk but it does change your symptoms. So, don’t expect Delta Long COVID symptoms to match Omicron.)
That puts your combined risk at around 55% after two infections and I assume your entropy recovery time will be slower because you have layered damage on to damage.
This is becoming a greater issue when many have suffered three or four infections.
The main problem in discerning risk reduction post-infection is that the entropy rate will be non-constant AND unique to each person based on but not limited to… health, immunity, and type of infection…
Allowing for a giant spectrum of possible recovery times.
But that’s not really relevant if you aren’t going long enough between infections.
It’s basically splitting hairs.
If you have four infections in a year, you will likely never reset your risk and it reaches 99.999% exceptionally fast… Even if that just means picking up one new symptom from each infection… Four symptoms later and you’re a full long hauler.
And almost certainly whatever chronic illness you may experience will be exacerbated.
It’s almost like to not experience some element of being a long hauler you have to win significant odds if you plan to sustain regular infections. That’s quite the gamble.
It’s actually the same chart.
You may remember that I mentioned that the risk of Long COVID and the risk of death is actually the same chart?
Well, we could arbitrarily put a red line at the 150% mark and call that death.
The reason we can arbitrarily put it there is that by that time your quality of life is so devastated that you will be a completely different person… Killing the ‘old’ you.
Actual death is not excluded from the list of potential outcomes.
And this would happen in a lot of ways but the main idea is that your body would be worn down from constant attacks as it’s being pulled apart cell by cell.
Which there is really no upside to. The inevitable fact is that with enough COVID infections you will die eventually. Even under the best circumstances.
And the only way to prevent Long COVID or Death from COVID?
Is not to sustain an infection, especially not multiple infections in a short amount of time.
I mentioned it wouldn’t alter the risk if you changed the numbers…
Since the initial risk is so high and the greatest risk happens at the start…
This is a rare instance where theory alone is sufficient to explain the entire risk.
That means if we fudge the numbers and say it’s 20% we only gain space for one or maybe two infections… Starting with 30% in the first 25 days means that we cannot sustain multiple infections in a short amount of time and since folks are seeing reinfections between 30-90 days and are likely still before the start of their recovery entropy for their risk from the first infection…
Then we are not only marching folks toward Long COVID but death as well.
Conclusion
We cannot live with COVID, there is no way to try to make COVID seasonal, and it means that an approach that treats COVID like Smallpox or Polio is required.
Long COVID is already having a devastating impact on our society. A study estimating the amount of new ME/CFS gave us some shocking results.
This was based on 25% for Long COVID and 5% for ME/CFS which is essentially fully disabled. An estimated 30+ Million people are suffering from Long COVID in the US.

But our troubles don’t stop there…
I mentioned earlier in the article that I would explain another reason that isolation is important… COVID is from the same grouping as SARS and when SARS was being tested on mice, which are a perfect scale for humans in regards to our brains… It’s even a joke in Hitchhiker’s Guide to the Galaxy… That after 15 “pass-throughs” SARS would mutate to become deadly to the 16th mouse.
This could very well have repercussions with COVID and NOONE has tested it.
And based on our anecdotal evidence after two years of the pandemic, we have a pretty clear idea that this is the nature of this virus. It even likely defines the wave structure we see… which would be defined by the incubation window and how quickly we get to 15 pass-throughs or in other words our mitigations or ability to isolate.
Now that the incubation window has shortened to three days, it’s three times as fast, and when you include reduction of mitigations… I don’t think that could be calculated.
But it’s bad and we are seeing new subvariants emerge all over the world.
So, if we allow COVID to roam freely and pass through as many hosts as possible, we are likely to develop a new even more deadly variant when our hospitals are weakened.
The more hosts it goes through the faster it develops.
This is why abandoning isolation is foolish… We isolate to prevent the mutations happening inside of us from escaping and being allowed to continue to mutate.
The more they mutate the deadlier they get… We must stop transmission.
We’re getting close to 5% of the world having Long COVID.

But we are also getting a better idea of what the actual infection timing really is.
At the start of Omicron, I thought that 18-day reinfections were possible but it’s far more likely that they are simply experiencing their 14-day resurgence…
But those 30-day reinfections? Those are likely actual acute reinfections, as they restart their acute phase. And we are seeing a ton of them.
Specifically from our schools.
It’s even possible that they are sustaining back-to-back infections with multiple variants per infection which would have horrible outcomes and blow all this theory out the window because it would lead to much worse situations.
We have already done untold damage to our youth that we will not identify for another five to ten years… From cancers to reproductive issues much later in life.

The thing that no one is saying is all this scarring from COVID removing our cells is essentially the process that also creates the environment for cancer cells to develop.
We say inflammation, but we should say scarring to better identify the risk.
But even now looking at the chart I displayed to demonstrate the length of infection, one could easily argue that the length of infection is 42 days and that puts risk closer to 36%… but this makes a great point… Adding 1/3 more days only added 6% risk because you create the most risk in the first few days of infection.
So, if folks want to split hairs over the initial risk percentage… You are still only talking about adding one or two infections to your total.
Plus, that 80% number is stagnant for every infection individually.
And it likely subsequently increases with each infection.
Bottom line risk for Long COVID?
80% risk of one symptom on each infection increasing after each infection.
30% risk of multiple symptoms on each infection increasing after each infection.
That risk also compounds if you do not have sufficient recovery time.
Four infections in a year mean that you are likely to have Long COVID or worse.
This all means the risk is very high, keep in mind some folks are up to 4 or 5 infections already… and because of the brain inflammation COVID is causing, there is an extremely high-risk level to both developing Long COVID or eventually death.
Remember, your first infection was likely asymptomatic but still included brain inflammation… It’s so important to explain that even an infection that does not invade the brain causes brain inflammation because of the cytokine response.
That Brain Inflammation is also causing encephalitis, doing something we see in concussion patients or TBIs where they experience personal risk index reduction.
If a person does have their brain invaded then there are somewhere between three and five forms of inflammation total with a whole host of new and very specific problems.
Now it is more important than ever to wear a high-quality, tightly fitting mask.
But beyond that? Keep an eye out.
We are seeing symptoms that look like these which can be advanced warning signs.

So, if you see someone who has recently been through a COVID infection and is telling folks that the risk is low… Or sending any of those warning signs…
We should treat them just like we would a concussion patient.
And right now, that’s all of our world leaders.
If you ever at any point, took your mask off then you were at risk for brain invasion.
I hope this article has helped you understand your risk a bit better.
You can follow me on Twitter @ https://twitter.com/DonEford
If you want to donate to my continued work…
You can do so here… DONATE.
But now…
Let’s talk about how I healed my minor Long COVID.
(Update: This is going to get moved to its own supplementary article as I have a GREAT deal of information to add to it. Hopefully, I can do it soon.)
Let’s be honest, we have a long way to go… and I am in no way affiliated with any products I’m going to suggest… Also, it’s all low risk… and OTC available.
Nothing I’m going to suggest here is medicine you would be prescribed by a doctor. As a strategist, it’s not my job to prescribe pharmaceuticals… but there are some big advances on the horizon… and it’s all made for humans.
First off, very few things have been proven to help with COVID that are OTC.
Zinc, Vitamin D, Specific Probiotics, and CBD oil… Have all held up under test.
The probiotic featured in this study is a combination of two probiotics, one of which is available over the counter. It just happened to be in the one I was using.
Lactiplantibacillus plantarum is the name of the actual probiotic.
I was using this particular brand.
When it comes to diet, I cannot stress enough the need for a low inflammation diet regarding all things COVID. For some reason in America, the government is not allowed to say that the food you eat matters unless it’s in the shape of a pyramid.
I regularly used this product as a drink that combined a lot of the vitamins that have been used in hospital settings… and rotating between that water and Orange Juice.
This study shows how CBD oil has amazing potential for blocking the virus and should help folks clean out any lingering virus.
This comes with a lot of caveats and is by no means a “miracle cure.” I share it based on my personal experience and the correlation between my single use of it and the clearance of my sixteen-month-long symptom… but every COVID infection is slightly different and every body is different.
The goal in any recovery is to create a new stable line for daily quality of life when charted out over the month.
There is no guarantee that it will resolve them, but it is shown to help in some cases.
As a late to the party edit, more information recently came out supporting that a lot of Long COVID symptoms can be related to the Vagus nerve which is the nerve that goes from your brain to your stomach.
(Update: this has been successfully used to reduce symptoms.)
This can be associated with symptoms relating to “persistent voice problems, difficulty swallowing, dizziness, abnormally high heart rate (tachycardia), low blood pressure, and digestive issues.”
In 2019, it was discovered that there is a non-invasive way to stimulate the Vagus nerve and it had a lot of success at removing vertigo and headaches.
I thought it was worth looking into since it is non-invasive… So, the risk is very low.
Now, this is usually the part where someone suggests exercise.
This has become somewhat controversial, especially in chronic illness communities.
So, it’s important to say that, technically, walking is enough and that is not controversial to say… You need sun and to walk outside. You cannot fully supplement the natural Vitamin D your body creates as a natural steroid.
You need all this plus time… Be patient with yourself.
There will never be a pill that completely stops Long COVID unless it stops infection of the virus. Though the Pfizer drug does show a lot of promise for helping with viral clearance and a whole host of actual treatments are on the way.
We are all going to have to be patient with ourselves as we heal, healing takes time.
And sometimes, time is all we got.
There is a surge of hopelessness and we have to resist that feeling.
It’s so important that we remember that we have a clearer idea of how to end the pandemic than ever and VERY smart people are working on it.
Please, if you need help, call someone, talk to someone, and do not rush to action.

This was very well-explained and I learned a lot. Thanks for using the graphs and simple language to communicate the nefarious effects of Covid. No... it's not the flu.
Thank you so much for this! I have shared with people who are a. important to me & b. because I really want them to understand what I've been screaming into the wind for quite some time! I am a brewery/restaurant owner and have continued to keep the inside of my restaurant closed! I am at moral and financial crossroads but I value the health of my staff, guests and friends more than $$. The only thing keeping us going is that we have a large outdoor beer garden. I live in Missouri, so the winter months have been brutal and every restaurant nearby has opened to full capacity inside. It terrifies me to no end. Your information absolutely helps me in sticking to my guns related to mitigation of risk/exposure/ and the need (at all cost) to avoid re-exposure. I could go on, but you have a dedicated follower in me and I look forward to (with some dread ;( ..) to more information from you.