Brace for Impact: 7/6/26
And Nuvaxovid vs mRNA part 2.

Brace for Impact is every Monday and Thursday, covering news, science, and public health from a progressive COVID-conscious perspective.
We’ve been doing twice-weekly updates on Trump’s failed presidency, the problematic antics of RFK Jr., the situation in Iran, developing public health issues, new Long COVID science, and whatever else is going on that you should know about.
It can be listened to on Twitter…

Or on YouTube…
mRNA vs Nuvaxovid for COVID Part 2
In the introduction of this slide deck, I’m trying to start with a simple argument…
Context is everything.
How we measure reality creates context.
And if we choose to measure reality with specific constraints, then it might limit what is perceived as true.
In this case, we are posing limitations on measuring Novavax in a way that benefits mRNA; sometimes this appears intentional, other times coincidental.
The general idea is that while mRNA is creating the context, it’s not actual reality.
And it’s not unfair to say that if you assess all that matters to most regulatory committees, they can easily be made to look the same, maybe even give mRNA an edge; this is the point I make on the left side of the panel.
On paper, we see that both mRNA and Novavax elicit similar responses, with the third shot maxing out the immune potential and the fourth shot returning it to baseline.
If you stopped measuring there, then they are the same.
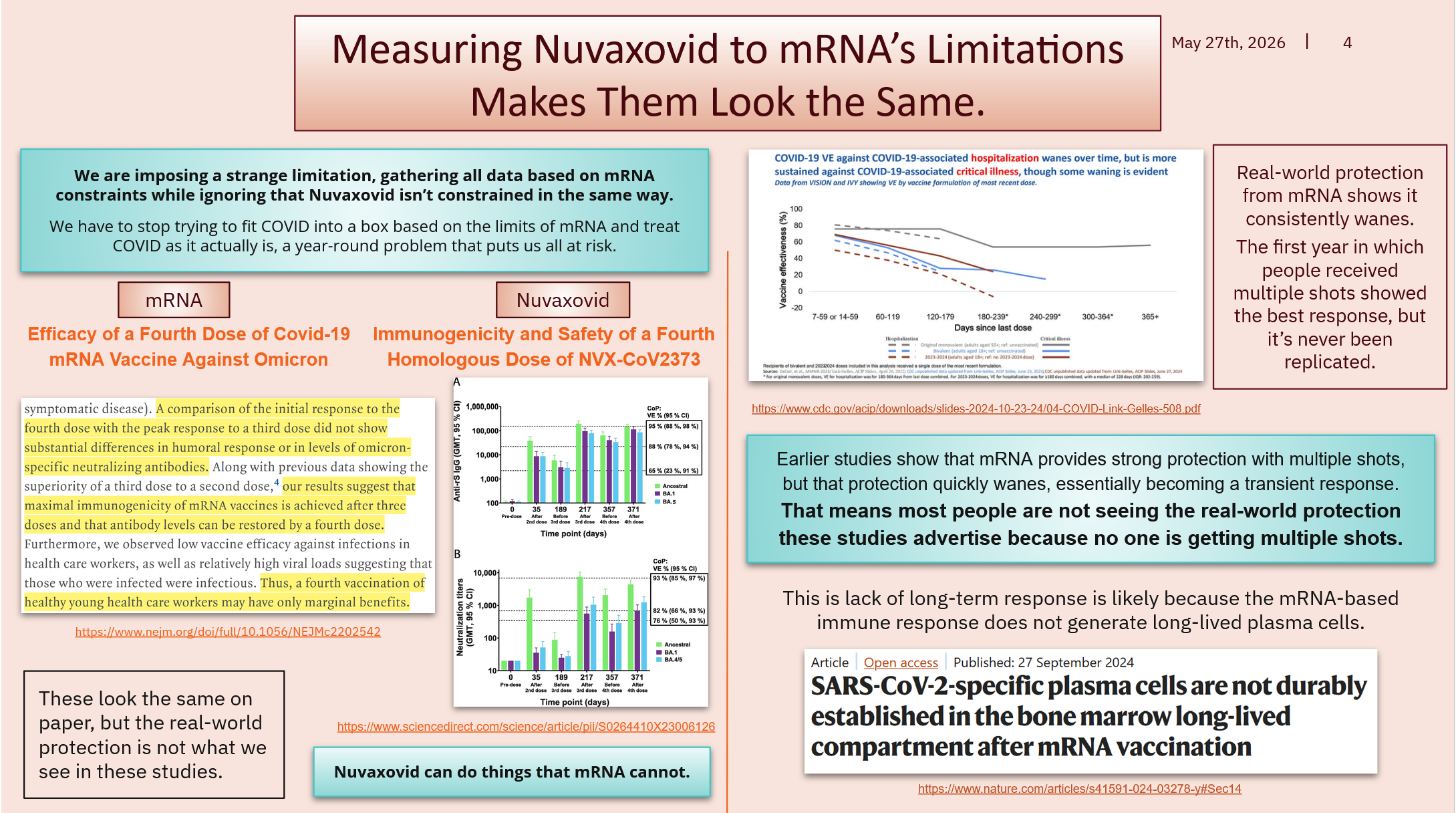
If you look to the right side of the chart, you will see the CDC data on the real-world effectiveness of mRNA… and the first year did show consistent results…
However, every year since has only given about half a year of waning protection.
This is happening because mRNA wanes to nothing and doesn’t build on subsequent shots… It’s starting over again every year; it’s not really a booster at this point.
They are using data that was only good for that single year because no one is getting multiple shots anymore, so that real-world protection is not occurring as stated.
And people shouldn’t be getting multiple shots every year for a variety of reasons that will be covered in later slides, but this is the US government's consensus.
You’re probably thinking, “But I heard these have high efficacy?”
If you are confused, that’s because efficacy and effectiveness are not the same thing in these usages… efficacy is the testing results; effectiveness is the real-world protection.
Efficacy can be good or bad depending on the parameters of your testing or how the study decides to measure reality. We hear them say it has excellent efficacy or desired results, which are subjective concepts; it’s not relative to other products unless they use the “non-inferiority” reference point, which can still be flexible.
Real-world effectiveness is the objective reality, or as close as we can get using models based on real-world data.
We can use standard measurements to create objective comparisons, while most vaccine manufacturers seeking approvals prefer comparators. This allows them to choose a specific, similar vaccine to compare against, giving themselves the appearance of higher performance.
It’s like picking a boxer weaker than you to prove you’re a better fighter.
It feels like it’s relative based on usage, but efficacy depends on unique testing parameters. An example of this is that mRNA tests aim to prevent hospitalization, while Nuvaxovid tests aim to prevent infection, but both can have equal efficacy because they both met their desired outcomes… or they can both have protection levels that use similar numbers but mean vastly different things.
To make things more confusing, mRNA also elicited an upper respiratory tract response with the initial doses, which might have temporarily blocked infection. However, it hasn’t been able to replicate that response with subsequent shots. So, this is another layer to the onion on why using data from the first year is misleading.
Any way you want to look at it, using 2021-22 data for now is essentially fraud.
People will argue memory responses, or mature B cells, and that’s all true… But that’s almost the same as arguing for infection-based immunity.
What we want to see are called LLPC or long-lived plasma cells of the bone marrow.
mRNA famously does not create LLPCs, and Nuvaxovid does because of Matrix-M.
While the marketing or social media personalities will claim that the protection offered in the first year is what you get now, that’s simply false advertising.
So, if we stop measuring objective reality and limit ourselves to a subjective reality based on mRNA’s limitations, then sure, they are the same.
But that’s not actual reality, and it’s certainly not the best way to protect yourself in an active pandemic; that’s a marketing hellscape that gives everyone Long COVID, and we just got another study showing that the risk of LC in children is not reduced after mRNA vaccination…

We need pediatric Nuvaxovid expansion right away…
It’s especially frustrating knowing it's the same vaccine that I will get in the fall that my children will use when it’s finally approved.
The vaccine they need is literally available, but we can’t access it for them.
We should be more outraged.
Call to action.
Public comment closes on July 13th.

A lot of people have tried many different repurposed drugs for Long COVID, and while most have failed, that isn’t always the case. Sometimes it works.
And if you want to see the benefit you experienced extended to others…
This is your chance.
The deadline has already been extended once, and now you have until July 13th.
Personally, I’d like to see more mAbs from previous variants, or Invivyd’s infusion treatment for COVID prevention, repurposed for Long COVID.
We proved in 2022 that persistence is driving a large portion of the disease, and this particular feature is degenerative, meaning it is the most dangerous aspect.
And while it’s good you can use Nuvaxovid every two months, the persistent variants from cases early in the pandemic are too far away from the antibodies we’re training our immune system to protect us from now.
That means we need to repurpose older vaccine antigens or infusion antivirals that are currently approved only for treating acute COVID or preventing it.
If you don’t know what to write as a public comment, leave a comment here, and we can help you gain the confidence needed to write a simple but effective comment.
If you would like to support our work, please consider becoming a paid subscriber.
Or if you’d prefer, you can also make a one-time contribution at this link.
